Q1. Which kind of agent has no evidence of clinical benefit in the treatment of Waldenstrom’s macroglobulinemia?¶
- (A) Proteosome inhibitor
- (B) BTK inhibitor
- (C) Anti-CD20 monoclonal antibody
- (D) PI3K inhibitor
- (E) Alkyating chemotherapy
點此顯示正解
(D) PI3K inhibitor
詳解¶
1. Why (D) PI3K inhibitor is the CORRECT answer (has NO evidence of clinical benefit)¶
(D) PI3K inhibitor is the correct answer because PI3K inhibitors have no established clinical benefit in Waldenstrom macroglobulinemia (WM). While preclinical studies demonstrated that PI3K pathway inhibition has theoretical rationale in WM[9][11], clinical trials have been disappointing and terminated early due to toxicity without establishing efficacy:
- A phase 2 study of idelalisib (PI3K-delta inhibitor) in WM was terminated early after only 5 patients were enrolled due to grade 3 or worse hepatotoxicity in 3 of the first 5 patients7
- A small phase 1/2 study showed 80% response rate in 10 patients, but the combination of idelalisib plus obinutuzumab had 50% premature discontinuation due to toxicity and 25% developed elevated liver enzymes7
- PI3K inhibitors are not mentioned in any consensus treatment guidelines for WM, including the Tenth International Workshop for Waldenström Macroglobulinaemia consensus recommendations13, Mayo mSMART guidelines6, or recent reviews25
2. Why the OTHER options DO have evidence of clinical benefit¶
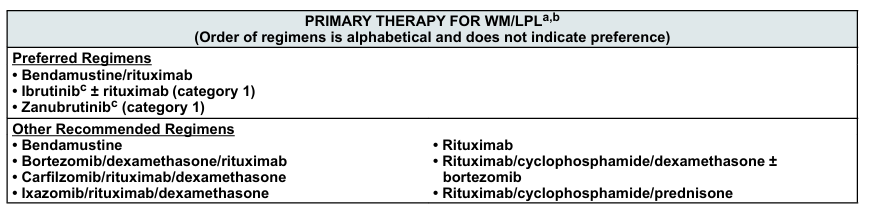
(A) Proteasome inhibitor - INCORRECT choice (has established benefit): - Proteasome inhibitors (bortezomib, carfilzomib, ixazomib) in combination with rituximab are preferred first-line therapy options per consensus guidelines13 - Bortezomib-dexamethasone-rituximab (BDR) is specifically listed as a preferred treatment regimen36 - Multiple guidelines recommend proteasome inhibitor-based regimens for both newly diagnosed and relapsed/refractory WM145
(B) BTK inhibitor - INCORRECT choice (has established benefit): - BTK inhibitors are among the most well-established therapies for WM124 - Ibrutinib is FDA-approved for WM and listed as a preferred first-line option (alone or with rituximab)13 - Zanubrutinib was approved in 2021 for WM and is preferred at Mayo Clinic due to better toxicity profile than ibrutinib25 - The INNOVATE trial demonstrated that ibrutinib plus rituximab significantly improved progression-free survival2
(C) Anti-CD20 monoclonal antibody - INCORRECT choice (has established benefit): - Rituximab (anti-CD20 antibody) is a cornerstone of WM therapy14[^10] - Rituximab-based combinations are the most widely used regimens in WM management[^10] - Bendamustine plus rituximab and cyclophosphamide-dexamethasone-rituximab are preferred first-line options135 - All major guidelines recommend rituximab-containing regimens6
(E) Alkylating chemotherapy - INCORRECT choice (has established benefit): - Alkylating agents (bendamustine, cyclophosphamide) combined with rituximab are established first-line therapy options per consensus guidelines12 - Bendamustine-rituximab is a preferred regimen and commonly used at Mayo Clinic35 - Cyclophosphamide-dexamethasone-rituximab (CDR/DRC) is widely recommended36[^10]
詳解 · 中文翻譯¶
1. 為何 (D) PI3K 抑制劑是正確答案(在臨床治療中無益處證據)¶
(D) PI3K 抑制劑 是正確答案,因為 PI3K 抑制劑在 Waldenström 巨球蛋白血症(WM)中無既定臨床益處。儘管臨床前研究證明 PI3K 通路抑制在 WM 中有理論基礎[9][11],臨床試驗因毒性而令人失望並提前終止,未能確立療效:
- idelalisib(PI3K-delta 抑制劑)在 WM 中的第 2 期研究在僅招募 5 名患者後因第一個 5 名患者中的 3 名出現第 3 級或更高肝毒性而 提前終止7
- 一項小型第 1/2 期研究在 10 名患者中顯示 80% 反應率,但 idelalisib 加 obinutuzumab 的組合有 50% 過早停用因毒性和 25% 發展升高的肝酶7
- PI3K 抑制劑未在 WM 的任何共識治療指南中提及,包括第十國際 Waldenström 巨球蛋白血症研討會共識建議13、Mayo mSMART 指南6或最近評論25
2. 為何其他選項確實有臨床益處證據¶
(A) 蛋白酶體抑制劑 - 不正確選擇(具有既定益處): - 蛋白酶體抑制劑(bortezomib、carfilzomib、ixazomib)與 rituximab 組合是 共識指南首選一線治療選項13 - Bortezomib-地塞米松-rituximab(BDR)特別被列為首選治療方案36 - 多項指南對新診斷和復發/難治 WM 推薦蛋白酶體抑制劑基礎方案145
(B) BTK 抑制劑 - 不正確選擇(具有既定益處): - BTK 抑制劑位於 WM 最公認建立的治療中124 - Ibrutinib 對 WM FDA 批准,被列為首選一線選項(單獨或與 rituximab)13 - Zanubrutinib 在 2021 年獲批用於 WM,在 Mayo 診所因優於 ibrutinib 的毒性譜被偏好25 - INNOVATE 試驗證明 ibrutinib 加 rituximab 顯著改善無進展生存2
(C) 抗 CD20 單克隆抗體 - 不正確選擇(具有既定益處): - Rituximab(抗 CD20 抗體)是 WM 治療的基石14[^10] - Rituximab 基礎組合是 WM 管理中最廣泛使用的方案[^10] - Bendamustine 加 rituximab 和環磷酰胺-地塞米松-rituximab 是首選一線選項135 - 所有主要指南推薦含 rituximab 方案6
(E) 烷化化療 - 不正確選擇(具有既定益處): - 烷化代理(bendamustine、環磷酰胺)與 rituximab 組合是 共識指南既定一線治療選項12 - Bendamustine-rituximab 是首選方案,在 Mayo 診所常用35 - 環磷酰胺-地塞米松-rituximab(CDR/DRC)被廣泛推薦36[^10]
參考文獻 (AMA)¶
-
Sahin I, Azab F, Mishima Y, et al. Targeting Survival and Cell Trafficking in Multiple Myeloma and Waldenstrom Macroglobulinemia Using Pan-Class I PI3K Inhibitor, Buparlisib. American Journal of Hematology. 2014;89(11):1030-6. doi:10.1002/ajh.23814. PMID:25060991. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Roccaro AM, Sacco A, Husu EN, et al. Dual Targeting of the PI3K/Akt/mTOR Pathway as an Antitumor Strategy in Waldenstrom Macroglobulinemia. Blood. 2010;115(3):559-69. doi:10.1182/blood-2009-07-235747. PMID:19965685. ↩↩↩↩↩↩↩↩↩↩
-
Castillo JJ, Advani RH, Branagan AR, et al. Consensus Treatment Recommendations From the Tenth International Workshop for Waldenström Macroglobulinaemia. The Lancet. Haematology. 2020;7(11):e827-e837. doi:10.1016/S2352-3026(20)30224-6. PMID:33091356. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Kapoor P, Ansell SM, Fonseca R, et al. Diagnosis and Management of Waldenström Macroglobulinemia: Mayo Stratification of Macroglobulinemia and Risk-Adapted Therapy (mSMART) Guidelines 2016. JAMA Oncology. 2017;3(9):1257-1265. doi:10.1001/jamaoncol.2016.5763. PMID:28056114. ↩↩↩↩↩↩
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩↩↩↩↩↩↩↩↩
-
Gertz MA. Waldenström Macroglobulinemia: 2023 Update on Diagnosis, Risk Stratification, and Management. American Journal of Hematology. 2023;98(2):348-358. doi:10.1002/ajh.26796. PMID:36588395. ↩↩↩↩↩↩↩↩
-
Castillo JJ, Treon SP. What Is New in the Treatment of Waldenstrom Macroglobulinemia?. Leukemia. 2019;33(11):2555-2562. doi:10.1038/s41375-019-0592-8. PMID:31591468. ↩↩↩↩
-
Gavriatopoulou M, Terpos E, Kastritis E, Dimopoulos MA. Current Treatment Options and Investigational Drugs for Waldenstrom's Macroglobulinemia. Expert Opinion on Investigational Drugs. 2017;26(2):197-205. doi:10.1080/13543784.2017.1275561. PMID:28043164. ↩
Slide annotations
PRIMARY THERAPY FOR WM/LPL table provided as reference.
Figures¶