Q57. An 18-year-old male patient is diagnosed with Anaplastic Large Cell Lymphoma (ALCL). Initial workup reveals advanced-stage disease with B symptoms and skin involvement. Immunohistochemistry (IHC) staining shows tumor cells are CD30-positive, and ALK protein expression is positive in both the cytoplasm and nuclei. Which of the following statements concerning ALCL is least accurate?¶
- (A) ALK-positive ALCL typically presents in younger patients, with a median age at diagnosis of 15-30 years.
- (B) ALK expression holds both prognostic and predictive significance in ALCL, as ALK-positive ALCL is more chemosensitive than its ALK-negative counterpart, leading to higher complete remission rates and improved long-term survival.
- (C) In ALK-positive ALCL, the classic t(2;5) translocation is the most common ALK rearrangement, characterized by ALK protein expression that is positive in the cytoplasm but negative in the nucleus, distinguishing it from other variants.
- (D) The combination of Brentuximab vedotin (BV) with cyclophosphamide, Adriamycin, and prednisone (BV-CHP) has proven superior to CHOP alone in CD30-positive peripheral T-cell lymphoma (PTCL), including ALCL patients, making BV-CHP the preferred first-line treatment for ALCL.
- (E) Crizotinib, an oral ALK tyrosine kinase inhibitor, is FDA-approved for treating relapsed/refractory ALK-positive ALCL in children and young adults, and it has also demonstrated activity in adult patients.
點此顯示正解
(C) In ALK-positive ALCL, the classic t(2;5) translocation is the most common ALK rearrangement, characterized by ALK protein expression that is positive in the cytoplasm but negative in the nucleus, distinguishing it from other variants.
詳解¶
Answer to Board Question¶
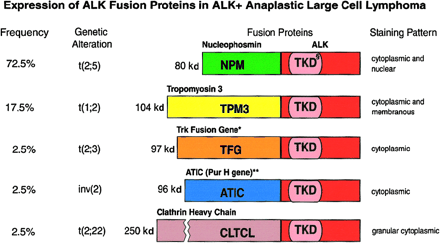
Statement (C) is FALSE because the classic t(2;5) translocation producing NPM-ALK fusion demonstrates both cytoplasmic AND nuclear ALK staining, not cytoplasmic-only staining. The NPM1 (nucleophosmin) protein normally shuttles between nucleus and cytoplasm, and when fused to ALK, the NPM1-ALK fusion protein retains this property, resulting in the characteristic dual nuclear and cytoplasmic staining pattern45. In contrast, variant ALK fusions (such as TPM3-ALK, ATIC-ALK, CLTC-ALK, and others) show cytoplasmic-only or membrane-restricted staining because their fusion partners lack nuclear localization signals245.
The immunohistochemical pattern is diagnostically important: NPM1-ALK shows both nuclear and cytoplasmic positivity, while variant fusions show cytoplasmic-only patterns. One study noted that "in lymphomas expressing NPM-ALK...cytoplasmic as well as nuclear labeling is seen," whereas variant ALK fusions show "ALK staining restricted to the cytoplasm"5. Another review confirmed that "the classical NPM1-ALK translocation leads to nuclear and cytoplasmic ALK staining," while other translocations like t(1;2) cause "ALK protein accumulation only in the cytoplasm"4.
Why the other statements are TRUE:
(A) TRUE: ALK-positive ALCL predominantly affects younger patients, with median age at diagnosis typically 15-30 years, in contrast to ALK-negative ALCL which occurs in older adults (median age 55-60 years)4.
(B) TRUE: ALK expression has both prognostic and predictive significance. ALK-positive ALCL demonstrates superior chemosensitivity compared to ALK-negative disease, with higher complete remission rates (70-90% vs 40-65%) and significantly better 5-year overall survival (70-90% vs 33-49%)45. The excellent prognosis of ALK-positive ALCL is "clearly different from that of ALK-negative anaplastic large-cell lymphomas"5.
(D) TRUE: The ECHELON-2 trial demonstrated that brentuximab vedotin plus CHP (BV-CHP, also called A+CHP) is superior to CHOP in CD30-positive PTCL, including ALCL. The trial showed median progression-free survival of 48.2 months with BV-CHP versus 20.8 months with CHOP (HR 0.71), with improved overall survival (HR 0.66) and higher complete response rates (68% vs 56%)6[7][8]. For the systemic ALCL subset specifically, the hazard ratio for progression-free survival was 0.59 (95% CI 0.42-0.84)[^7]. This led to FDA approval in 2018, making BV-CHP the preferred first-line treatment for CD30-positive PTCL including ALCL[^8].
(E) TRUE: Crizotinib, an oral ALK tyrosine kinase inhibitor, received FDA approval for relapsed/refractory ALK-positive ALCL in pediatric and young adult patients. The drug has demonstrated significant activity in both pediatric and adult populations with relapsed/refractory disease, with objective response rates of 80-90% in clinical trials4.
詳解 · 中文翻譯¶
血液委員會試題答案¶
敘述 (C) 錯誤,因為經典的 t(2;5) 易位產生的 NPM-ALK 融合蛋白展現細胞質和核內 ALK 著色,而非僅細胞質著色。NPM1(核磷蛋白)正常在核與細胞質間穿梭,當與 ALK 融合時,NPM1-ALK 融合蛋白保留此特性,導致特徵性雙核內和細胞質著色型態45。相對地,變異型 ALK 融合(如 TPM3-ALK、ATIC-ALK、CLTC-ALK 等)顯示 僅細胞質或膜限制著色,因為其融合伙伴缺乏核定位信號245。
免疫組織化學型態在診斷上很重要:NPM1-ALK 顯示核內和細胞質陽性,而變異型融合顯示僅細胞質型態。一項研究指出「在表達 NPM-ALK 的淋巴瘤中...可見細胞質及核著色」,而變異型 ALK 融合顯示「ALK 著色限制於細胞質」5。另一評論確認「經典 NPM1-ALK 易位導致核內和細胞質 ALK 著色」,而其他易位如 t(1;2) 導致「ALK 蛋白僅在細胞質中蓄積」4。
為何其他敘述正確:
(A) 正確:ALK 陽性 ALCL 主要影響較年輕患者,診斷時中位年齡通常 15-30 歲,與發生於年長成人(中位年齡 55-60 歲)的 ALK 陰性 ALCL 形成對比4。
(B) 正確:ALK 表達具有預後和預測意義。ALK 陽性 ALCL 相比 ALK 陰性疾病展現優越的化療敏感性,完全緩解率更高(70-90% vs 40-65%)且 5 年整體存活率明顯較佳(70-90% vs 33-49%)45。ALK 陽性 ALCL 的優異預後「明顯不同於 ALK 陰性非霍奇金淋巴瘤的預後」5。
(D) 正確:ECHELON-2 試驗證示 brentuximab vedotin 加 CHP(BV-CHP,亦稱 A+CHP)優於 CHOP 在 CD30 陽性周邊 T 細胞淋巴瘤(PTCL),包括 ALCL。試驗顯示 BV-CHP 的中位無進展存活期為 48.2 個月,versus CHOP 的 20.8 個月(HR 0.71),伴整體存活改善(HR 0.66)及更高完全應答率(68% vs 56%)6[7][8]。對於特定全身性 ALCL 子群,無進展存活期危害比為 0.59(95% CI 0.42-0.84)[^7]。這導致 2018 年 FDA 批准,使 BV-CHP 成為 CD30 陽性 PTCL(包括 ALCL)的首選一線治療[^8]。
(E) 正確:Crizotinib,一種口服 ALK 酪氨酸激酶抑制劑,獲得 FDA 批准用於兒科及年輕成人患者的復發/難治 ALK 陽性 ALCL。該藥物在復發/難治疾病的兒科和成人患者中展現顯著活性,臨床試驗中客觀應答率為 80-90%4。
參考文獻 (AMA)¶
-
Eyre TA, Khan D, Hall GW, Collins GP. Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma: Current and Future Perspectives in Adult and Paediatric Disease. European Journal of Haematology. 2014;93(6):455-68. doi:10.1111/ejh.12360. PMID:24766435. ↩
-
Falini B, Pulford K, Pucciarini A, et al. Lymphomas Expressing ALK Fusion Protein(s) Other Than NPM-ALK. Blood. 1999;94(10):3509-15. PMID:10552961. https://pubmed.ncbi.nlm.nih.gov/10552961. ↩↩
-
Zhu T, Zhou CJ, Jin L, et al. Clinical Characteristics and Prognostic Analysis of Non-Npm1-Alk Fusions in Pediatric Patients With ALK-Positive Anaplastic Large-Cell Lymphoma: A Single-Center Retrospective Study in China. Pediatric Blood & Cancer. 2026;73(2):e70045. doi:10.1002/1545-5017.70045. PMID:41431141. ↩
-
Horwitz S, O'Connor OA, Pro B, et al. The ECHELON-2 Trial: 5-Year Results of a Randomized, Phase III Study of Brentuximab Vedotin With Chemotherapy for CD30-positive Peripheral T-Cell Lymphoma. Annals of Oncology : Official Journal of the European Society for Medical Oncology. 2022;33(3):288-298. doi:10.1016/j.annonc.2021.12.002. PMID:34921960. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Horwitz S, O'Connor OA, Pro B, et al. Brentuximab Vedotin With Chemotherapy for CD30-positive Peripheral T-Cell Lymphoma (ECHELON-2): A Global, Double-Blind, Randomised, Phase 3 Trial. Lancet (London, England). 2019;393(10168):229-240. doi:10.1016/S0140-6736(18)32984-2. PMID:30522922. ↩↩↩↩↩↩↩↩↩↩
-
Richardson NC, Kasamon YL, Chen H, et al. FDA Approval Summary: Brentuximab Vedotin in First-Line Treatment of Peripheral T-Cell Lymphoma. The Oncologist. 2019;24(5):e180-e187. doi:10.1634/theoncologist.2019-0098. PMID:30914464. ↩↩
Slide annotations
Expression of ALK Fusion Proteins in ALK+ Anaplastic Large Cell Lymphoma table provided as reference.
Figures¶