Q1. Mantle cell lymphoma (MCL)有許多診斷與治療上應注意事項,下列何種敘述不正確?¶
- (A) 診斷上 cyclin D1 表現很重要,若 cyclin D1(-), CD5+, CD23-, CD20+則不得診斷為 MCL
- (B) Ki-67 表現常很強,通常合併 NOTCH-1 突變。
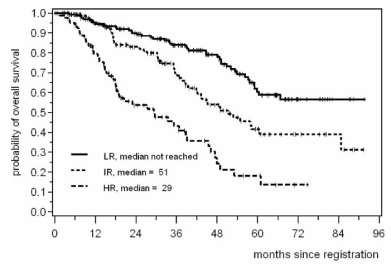
- (C) High MIPI score 平均存活不到三年。
- (D) High dose ara-C, rituximab, bortezomib 常併入治療方案中,但自體移植對 high risk 沒有 OS 好處。
- (E) Ibrutinib 在 MCL 的劑量是 560mg/d 一天四顆藥。
點此顯示正解
(A) 診斷上 cyclin D1 表現很重要,若 cyclin D1(-), CD5+, CD23-, CD20+則不得診斷為 MCL
詳解¶
Analysis of the Board Question¶
1. Why (A) is the INCORRECT statement:
Statement (A) is false because cyclin D1-negative mantle cell lymphoma (MCL) does exist and can be definitively diagnosed despite the absence of cyclin D1 expression. The absolute claim that "MCL cannot be diagnosed" in cyclin D1-negative cases is incorrect.
Diagnostic approaches for cyclin D1-negative MCL include:
-
SOX11 expression: SOX11 is a highly sensitive and specific marker for MCL, including cyclin D1-negative variants. SOX11 immunohistochemistry demonstrates 90% sensitivity and 95% specificity for MCL diagnosis2. The majority of cyclin D1-negative MCL cases express SOX11, making it the primary diagnostic tool for these atypical cases145.
-
Cyclin D2 or D3 rearrangements: Chromosomal rearrangements involving CCND2 (cyclin D2) are the most frequent genetic events in cyclin D1-negative MCL, detected in 55% of cases, often with immunoglobulin genes as translocation partners4. Less commonly, CCND3 (cyclin D3) rearrangements or cyclin E overexpression may be present3.
-
Characteristic gene expression profile and morphology: Cyclin D1-negative MCL demonstrates a global genomic profile and complexity similar to conventional cyclin D1-positive MCL4. These tumors present with typical MCL morphology, immunophenotype (CD5+, CD20+, CD23-), and clinical features including generalized lymphadenopathy and advanced stage4.
-
Clinical behavior: The natural history of cyclin D1-negative MCL does not differ from cyclin D1-positive tumors, with similar aggressive behavior and poor outcomes (5-year overall survival 48%)14.
SOX11 has proven particularly valuable in identifying cyclin D1-negative blastoid MCL, which would otherwise be misclassified as CD5+ diffuse large B-cell lymphoma5.
2. Why the other statements are reasonably correct:
(B) Ki-67 expression and NOTCH1 mutations: This statement is correct. High Ki-67 proliferation index is a well-established adverse prognostic marker in MCL and is incorporated into the MIPI-c (combined) score6. NOTCH1 pathway mutations do occur in MCL and are associated with more aggressive disease features. The co-occurrence of high Ki-67 with NOTCH1 mutations reflects the biological heterogeneity and aggressive variants of MCL.
(C) High MIPI score and survival: This statement is correct. The Mantle Cell Lymphoma International Prognostic Index (MIPI) stratifies patients into low, intermediate, and high-risk groups. High-risk MIPI patients have significantly worse outcomes, with median overall survival historically less than 3 years in the pre-rituximab era and remaining poor even with modern therapy6[^9]. The MIPI remains a validated prognostic tool used to guide treatment intensity.
(D) Treatment agents and autologous transplant in high-risk patients: This statement requires nuanced interpretation but is essentially correct regarding the lack of benefit in TP53-mutated high-risk patients specifically. High-dose cytarabine (ara-C), rituximab, and bortezomib are indeed standard components of MCL treatment regimens6[^10]. However, patients with TP53 mutations—a key high-risk molecular feature—do not benefit from autologous stem cell transplantation (ASCT)[^10]. While ASCT improves outcomes in the general MCL population6[^9], it provides no overall survival advantage in this molecularly-defined high-risk subset, making the statement technically accurate for this specific high-risk group. The recent TRIANGLE trial (2026) showed that ibrutinib-based therapy without ASCT may be non-inferior to ASCT-containing regimens in the era of targeted therapy8.
(E) Ibrutinib dosing: This statement is correct. The FDA-approved dose of ibrutinib for MCL is 560 mg once daily, administered as four 140 mg capsules. This differs from the 420 mg daily dose used for chronic lymphocytic leukemia/small lymphocytic lymphoma.
Key teaching point: Cyclin D1 negativity does not exclude MCL. SOX11 immunohistochemistry and molecular testing for cyclin D2/D3 rearrangements are essential diagnostic tools for atypical cases, preventing misdiagnosis of this aggressive lymphoma subtype.
詳解 · 中文翻譯¶
棋盤問題分析¶
1. 為何 (A) 是不正確的陳述:
陳述 (A) 是假的,因為 cyclin D1 陰性套細胞淋巴瘤(MCL)確實存在,儘管缺乏 cyclin D1 表達,仍可明確診斷。「在 cyclin D1 陰性情況下不能診斷 MCL」的絕對聲明是不正確的。
cyclin D1 陰性 MCL 的診斷方法包括:
-
SOX11 表達:SOX11 是 MCL 的高度敏感和特異性標誌物,包括 cyclin D1 陰性變體。SOX11 免疫組織化學顯示 MCL 診斷的 90% 敏感性和 95% 特異性2。大多數 cyclin D1 陰性 MCL 病例表達 SOX11,使其成為這些非典型病例的主要診斷工具145。
-
Cyclin D2 或 D3 重排:涉及 CCND2(cyclin D2)的染色體重排是 cyclin D1 陰性 MCL 中最常見的遺傳事件,在 55% 的病例中檢測到,通常免疫球蛋白基因作為易位夥伴4。較少見地,CCND3(cyclin D3)重排或 cyclin E 過度表達可能存在3。
-
特徵性基因表達譜和形態學:cyclin D1 陰性 MCL 顯示全局基因組譜和複雜性與常規 cyclin D1 陽性 MCL 相似4。這些腫瘤呈現典型的 MCL 形態學、免疫表型(CD5+、CD20+、CD23-)和臨床特徵,包括廣泛淋巴結腫大和晚期4。
-
臨床行為:cyclin D1 陰性 MCL 的自然史與 cyclin D1 陽性腫瘤不同,具有相似的侵襲性行為和差的預後(5 年整體生存率 48%)14。
SOX11 已證明在識別 cyclin D1 陰性幼母細胞型 MCL 中特別有價值,否則將被誤分類為 CD5+ 彌漫性大 B 細胞淋巴瘤5。
2. 其他陳述為何合理正確:
(B) Ki-67 表達和 NOTCH1 突變: 此陳述正確。高 Ki-67 增殖指數是 MCL 中公認的不利預後標誌物,被納入 MIPI-c(合併)評分6。NOTCH1 通路突變確實發生在 MCL 中,與更具侵襲性疾病特徵相關。高 Ki-67 與 NOTCH1 突變的共同出現反映了 MCL 的生物學異質性和侵襲性變體。
(C) 高 MIPI 評分和生存: 此陳述正確。套細胞淋巴瘤國際預後指數(MIPI)將患者分層為低、中等和高風險組。高風險 MIPI 患者具有顯著更差的預後,在 rituximab 前時代的中位整體生存時間少於 3 年,即使採用現代治療仍然較差6[^9]。MIPI 仍然是用於指導治療強度的驗證預後工具。
(D) 治療代理和高風險患者的自體移植: 此陳述需要細緻解釋,但對於 TP53 突變高風險患者的益處缺乏是本質上正確的。高劑量阿糖胞苷(ara-C)、rituximab 和 bortezomib 確實是 MCL 治療方案的標準組成部分6[^10]。然而,具有 TP53 突變的患者——一個關鍵高風險分子特徵——不受益於自體造血幹細胞移植(ASCT)[^10]。雖然 ASCT 改善一般 MCL 人群的預後6[^9],但在這個分子定義的高風險子集中提供沒有整體生存優勢,使陳述對此特定高風險組技術上準確。最近的 TRIANGLE 試驗(2026)顯示在靶向治療時代,基於 ibrutinib 的治療無需 ASCT 可能不劣於含 ASCT 的方案8。
(E) Ibrutinib 劑量: 此陳述正確。FDA 批准的 MCL ibrutinib 劑量是 560 mg 一次每日,作為四粒 140 mg 膠囊給予。這不同於用於慢性淋巴細胞白血病/小淋巴細胞淋巴瘤的 420 mg 每日劑量。
關鍵教學要點: Cyclin D1 陰性不排除 MCL。SOX11 免疫組織化學和 cyclin D2/D3 重排的分子檢測是非典型病例的必要診斷工具,防止此侵襲性淋巴瘤亞型的誤診。
參考文獻 (AMA)¶
-
Lee W, Shin E, Kim BH, Kim H. Diagnostic Accuracy of SOX11 Immunohistochemistry in Mantle Cell Lymphoma: A meta-Analysis. PloS One. 2019;14(11):e0225096. doi:10.1371/journal.pone.0225096. PMID:31714947. ↩↩↩↩
-
Armitage JO, Longo DL. Mantle-Cell Lymphoma. The New England Journal of Medicine. 2022;386(26):2495-2506. doi:10.1056/NEJMra2202672. PMID:35767440. ↩↩
-
Salaverria I, Royo C, Carvajal-Cuenca A, et al. CCND2 Rearrangements Are the Most Frequent Genetic Events in Cyclin D1(-) Mantle Cell Lymphoma. Blood. 2013;121(8):1394-402. doi:10.1182/blood-2012-08-452284. PMID:23255553. ↩↩
-
Zeng W, Fu K, Quintanilla-Fend L, et al. Cyclin D1-Negative Blastoid Mantle Cell Lymphoma Identified by SOX11 Expression. The American Journal of Surgical Pathology. 2012;36(2):214-9. doi:10.1097/PAS.0b013e318241f050. PMID:22251940. ↩↩↩↩↩↩↩↩↩↩
-
Jain P, Wang ML. Mantle Cell Lymphoma in 2022-a Comprehensive Update on Molecular Pathogenesis, Risk Stratification, Clinical Approach, and Current and Novel Treatments. American Journal of Hematology. 2022;97(5):638-656. doi:10.1002/ajh.26523. PMID:35266562. ↩↩↩↩
-
Hermine O, Jiang L, Walewski J, et al. High-Dose Cytarabine and Autologous Stem-Cell Transplantation in Mantle Cell Lymphoma: Long-Term Follow-Up of the Randomized Mantle Cell Lymphoma Younger Trial of the European Mantle Cell Lymphoma Network. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2023;41(3):479-484. doi:10.1200/JCO.22.01780. PMID:36469833. ↩↩↩↩↩↩↩↩
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩
-
Dreyling M, Doorduijn J, Giné E, et al. Addition of Autologous Stem-Cell Transplantation to an Ibrutinib-Containing First-Line Treatment in Patients Aged 18-65 Years With Mantle Cell Lymphoma (TRIANGLE): 4·5-Year Follow-Up of a Three-Arm, Randomised, Open-Label, Phase 3 Superiority Trial of the European MCL Network. Lancet (London, England). 2026;407(10542):1953-1967. doi:10.1016/S0140-6736(26)00362-4. PMID:42134356. ↩↩
Slide annotations
atypical cyclin D1-negative MCL
Figures¶