Q1. 六十歲男性長期 3-4 年有 neutropenia, WBC 12,000/mm³, lymphocyte count 65%, Hb 8.0gm/dl, platelet 100K/mm³. 稍為會覺得累, 比較容易呼吸道感染。理學檢查沒有淋巴解腫大, 脾臟摸得到, 稍大。CD4+, CD3+, CD8-下列何項敘述為正確?¶
- (A) 1,2,3 正確
- (B) 1,3 正確
- (C) 2,4 正確
- (D) 4 正確
- (E) 以上皆正確
點此顯示正解
(E) 以上皆正確
詳解¶
The correct answer is (E) All of the above are correct because each of the four statements accurately reflects established features of T-cell large granular lymphocytic leukemia (T-LGLL).
Statement 1: Indolent course with good prognosis — TRUE
T-LGLL is consistently described as an indolent chronic lymphoproliferative disorder with a generally favorable prognosis2410. The disease typically affects older patients (median age ~66.5 years) and follows a chronic course2. While many patients eventually require treatment due to cytopenias or autoimmune complications, the majority experience an indolent clinical course, and deaths infrequently occur10. The disease is incurable but manageable, with most patients achieving long-term survival with appropriate supportive care and immunosuppressive therapy when indicated26.
Statement 2: STAT3 plays an important role (in ~30% of cases) — TRUE
STAT3 mutations are detected in approximately 28-40% of T-LGLL patients135. Multiple studies confirm this frequency: Barilà et al. found STAT3 mutations in 28.3% of 205 LGLL patients1, while other reports cite 30-40% prevalence3. These are somatic gain-of-function mutations, most commonly affecting the SH2 domain (particularly Y640F and N647I hotspot mutations), resulting in increased STAT3 dimerization, activation, and gene transcription35. STAT3 mutations are associated with more severe disease features including severe neutropenia (ANC <500/mm³), anemia, treatment requirement, and reduced overall survival1. The JAK-STAT pathway plays a key role in LGL pathogenesis by promoting survival, proliferation, and cytotoxicity24.
Statement 3: Often complicated by pure red cell aplasia (PRCA) — TRUE
PRCA is a well-recognized complication of T-LGLL89. In clinical practice, PRCA represents one of the major indications for treatment initiation in LGLL patients8. Liu et al. specifically studied 81 patients with LGLL-associated PRCA, demonstrating this is a common and clinically significant complication9. The NCCN guidelines list hemoglobin <10 g/dL or need for RBC transfusion as indications for treatment, reflecting the frequency of red cell aplasia in this population7. Treatment selection often considers PRCA status, with cyclosporine or cyclophosphamide preferred as first-line therapy for patients presenting with PRCA89.
Statement 4: Cyclophosphamide, cyclosporine, and cladribine all have good efficacy — TRUE
All three agents demonstrate good efficacy in T-LGLL treatment:
-
Cyclophosphamide: Highly effective with a 70% overall response rate as second-line therapy6. The NCCN guidelines list cyclophosphamide as a preferred first-line agent7. A recent phase III trial established cyclophosphamide 100 mg/day for 12 months as an effective regimen7. In PRCA-associated LGLL, cyclophosphamide-prednisone showed complete response rates of 53.8% and overall response rates of 84.6%9.
-
Cyclosporine: Listed as a preferred second-line agent in NCCN guidelines7 and recommended by Lamy and Loughran as an effective option when first-line therapy fails10. In PRCA patients, cyclosporine achieved complete response rates of 31-33% and overall response rates of 50-56%9.
-
Cladribine: A purine analogue specifically mentioned in NCCN guidelines as having been used successfully in LGLL7. The guidelines list "purine analogues" (including pentostatin, cladribine, and fludarabine) as preferred second-line therapy options7.
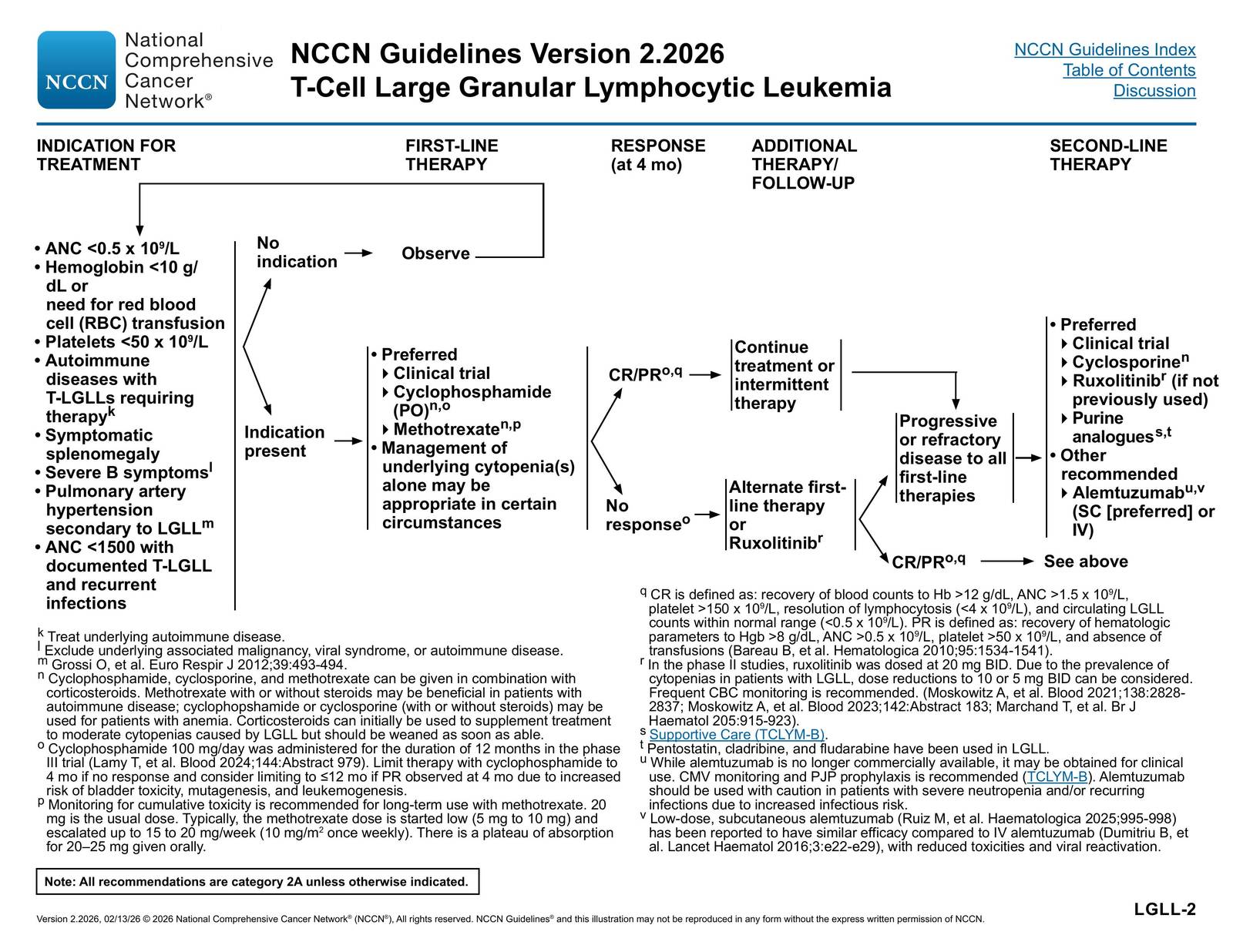
The NCCN T-Cell Lymphomas Guidelines algorithm above illustrates the treatment approach, showing cyclophosphamide and methotrexate as preferred first-line therapies, cyclosporine as preferred second-line therapy, and purine analogues (including cladribine) as additional second-line options7.
詳解 · 中文翻譯¶
正確答案是 (E) 以上皆正確因為四個敘述中每一個都準確反映了 T 細胞大顆粒淋巴細胞白血病(T-LGLL)的既定特徵。
敘述 1:惰性病程與良好預後 — 真實
T-LGLL 持續被描述為惰性慢性淋巴增生性疾病具有通常好的預後2410。病通常影響較老患者(中位年齡 ~66.5 歲)並遵循慢性病程2。雖然許多患者最終需要治療因為細胞減少症或自身免疫併發症,多數經歷惰性臨床病程,死亡鮮有發生10。病不可治癒但可管理,具有大多數患者以適當支持護理和適應免疫抑制療法成就長期生存26。
敘述 2:STAT3 在重要作用中發揮角色(於約 30% 的病例中) — 真實
STAT3 突變在約 28-40% 的 T-LGLL 患者中檢測到135。多項研究確認此頻率:Barilà 等人在 205 LGLL 患者中發現 STAT3 突變在 28.3% 中1,而其他報告引用 30-40% 流行率3。這些是體細胞增益功能突變,最常見影響 SH2 域(特別是 Y640F 和 N647I 熱點突變),導致增加的 STAT3 二聚化、激活和基因轉錄35。STAT3 突變與更嚴重的病特徵相關,包括嚴重中性粒細胞減少症(ANC <500/mm³)、貧血、治療需求和減少的總生存1。JAK-STAT 途徑在 LGL 病發病機制中發揮關鍵作用通過促進生存、增殖和細胞毒性24。
敘述 3:常被純紅細胞失不全(PRCA)複雜化 — 真實
PRCA 是 T-LGLL 的眾所周知的併發症89。在臨床實踐中,PRCA 代表 LGLL 患者中治療開始的主要適應之一8。Liu 等人特別研究了 81 名具有 LGLL 相關 PRCA 的患者,證實這是一個常見且臨床上顯著的併發症9。NCCN 指南列出血紅蛋白 <10 g/dL 或需要 RBC 輸血作為治療適應,反映此人口中紅細胞失不全的頻率7。治療選擇通常考慮 PRCA 狀態,具有環孢菌素或環磷酰胺偏好作為呈現具有 PRCA 患者的一線療法89。
敘述 4:環磷酰胺、環孢菌素和 cladribine 都具有好的療效 — 真實
所有三個製劑證示 T-LGLL 治療中的好療效:
-
環磷酰胺:高效具有 70% 總反應率作為二線療法6。NCCN 指南列出環磷酰胺作為偏好一線藥物7。最近第 III 期試驗建立環磷酰胺 100 mg/day 12 個月作為有效方案7。在 PRCA 相關 LGLL 中,環磷酰胺-潑尼松龍顯示完全反應率 53.8% 和總反應率 84.6%9。
-
環孢菌素:在 NCCN 指南中列為偏好二線藥物7並由 Lamy 和 Loughran 推薦作為有效選項當一線療法失敗時10。在 PRCA 患者中,環孢菌素達成完全反應率 31-33% 和總反應率 50-56%9。
-
Cladribine:嘌呤類似物特別在 NCCN 指南中提及已在 LGLL 中成功使用7。指南列出「嘌呤類似物」(包括 pentostatin、cladribine 和氟達拉濱)作為偏好二線療法選項7。
上述 NCCN T 細胞淋巴瘤指南演算法說明治療方法,顯示環磷酰胺和甲氨蝶呤作為偏好一線療法,環孢菌素作為偏好二線療法,嘌呤類似物(包括 cladribine)作為額外二線選項7。
參考文獻 (AMA)¶
-
Marchand T, Lamy T, Loughran TP. A Modern View of LGL Leukemia. Blood. 2024;144(18):1910-1923. doi:10.1182/blood.2023021790. PMID:38848524. ↩↩↩↩↩↩
-
Lamy T, Moignet A, Loughran TP. LGL Leukemia: From Pathogenesis to Treatment. Blood. 2017;129(9):1082-1094. doi:10.1182/blood-2016-08-692590. PMID:28115367. ↩↩↩↩↩↩↩↩
-
Lamy T, Loughran TP. How I Treat LGL Leukemia. Blood. 2011;117(10):2764-74. doi:10.1182/blood-2010-07-296962. PMID:21190991. ↩↩↩↩↩↩
-
Braunstein Z, Mishra A, Staub A, et al. Clinical Outcomes in T-Cell Large Granular Lymphocytic Leukaemia: Prognostic Factors and Treatment Response. British Journal of Haematology. 2021;192(3):484-493. doi:10.1111/bjh.16808. PMID:32519348. ↩↩↩↩
-
Barilà G, Teramo A, Calabretto G, et al. Stat3 Mutations Impact on Overall Survival in Large Granular Lymphocyte Leukemia: A Single-Center Experience of 205 Patients. Leukemia. 2020;34(4):1116-1124. doi:10.1038/s41375-019-0644-0. PMID:31740810. ↩↩↩↩
-
Chaimowitz NS, Smith MR, Forbes Satter LR. JAK/STAT Defects and Immune Dysregulation, and Guiding Therapeutic Choices. Immunological Reviews. 2024;322(1):311-328. doi:10.1111/imr.13312. PMID:38306168. ↩↩↩↩
-
Cheon H, Xing JC, Moosic KB, et al. Genomic Landscape of TCRαβ and TCRγδ T-Large Granular Lymphocyte Leukemia. Blood. 2022;139(20):3058-3072. doi:10.1182/blood.2021013164. PMID:35015834. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Dong N, Castillo Tokumori F, Isenalumhe L, et al. Large Granular Lymphocytic Leukemia - A Retrospective Study of 319 Cases. American Journal of Hematology. 2021;96(7):772-780. doi:10.1002/ajh.26183. PMID:33819354. ↩↩↩↩↩↩
-
Liu X, Chai X, Yu Q, et al. Clinical Features and Outcomes in Large Granular Lymphocyte Leukemia - associated Pure Red Cell Aplasia With STAT3 Mutation. Annals of Hematology. 2025;104(4):2351-2360. doi:10.1007/s00277-025-06371-5. PMID:40266290. ↩↩↩↩↩↩↩↩↩↩
-
National Comprehensive Cancer Network. T-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/t-cell.pdf#page=32. ↩↩↩↩↩↩
Slide annotations
indolent T-cell lymphoproliferative disorder (LPD) of the mature cytotoxic lymphocytes of effector memory cell phenotype. Most common: CD2, CD3, CD8, CD57, and TCRαβ. In rare cases, LGLLs are CD4+ alpha-beta T cells or gamma-delta T cells (CD8+ or CD4-/CD8-). There is significant clinical and pathophysiologic overlap with autoimmune syndromes, and in the majority of patients, LGLL is diagnosed concurrently with rheumatologic disease (ie, rheumatoid arthritis [RA] and systemic lupus erythematosus [SLE]).
Figures¶