Q1. Which one is incorrect for the management of multicentric Castleman disease (MCD)?¶
- (A) HHV8-associated MCD: The initial therapy is rituximab with mild symptoms. In the context of severe systemic symptoms or organ dysfunction consider etoposide in conjunction with rituximab.
- (B) POEMS-MCD: Should have standard myeloma induction therapy with consideration of consolidation with autologous HSCT.
- (C) Idiopathic MCD-TAFRO: Should receive parenteral corticosteroids and anti-IL-6 signalling therapy.
- (D) Idiopathic MCD, NOS, non-severe: Short course of corticosteroids only.
- (E) Idiopathic MCD, NOS, severe: If anti-IL-6 signalling therapy is not readily available or achieves an adequate response, it should be replaced by combination chemotherapy with rituximab-CHOP/CVP.
點此顯示正解
(D) Idiopathic MCD, NOS, non-severe: Short course of corticosteroids only.
詳解¶
Analysis of the Incorrect Statement¶
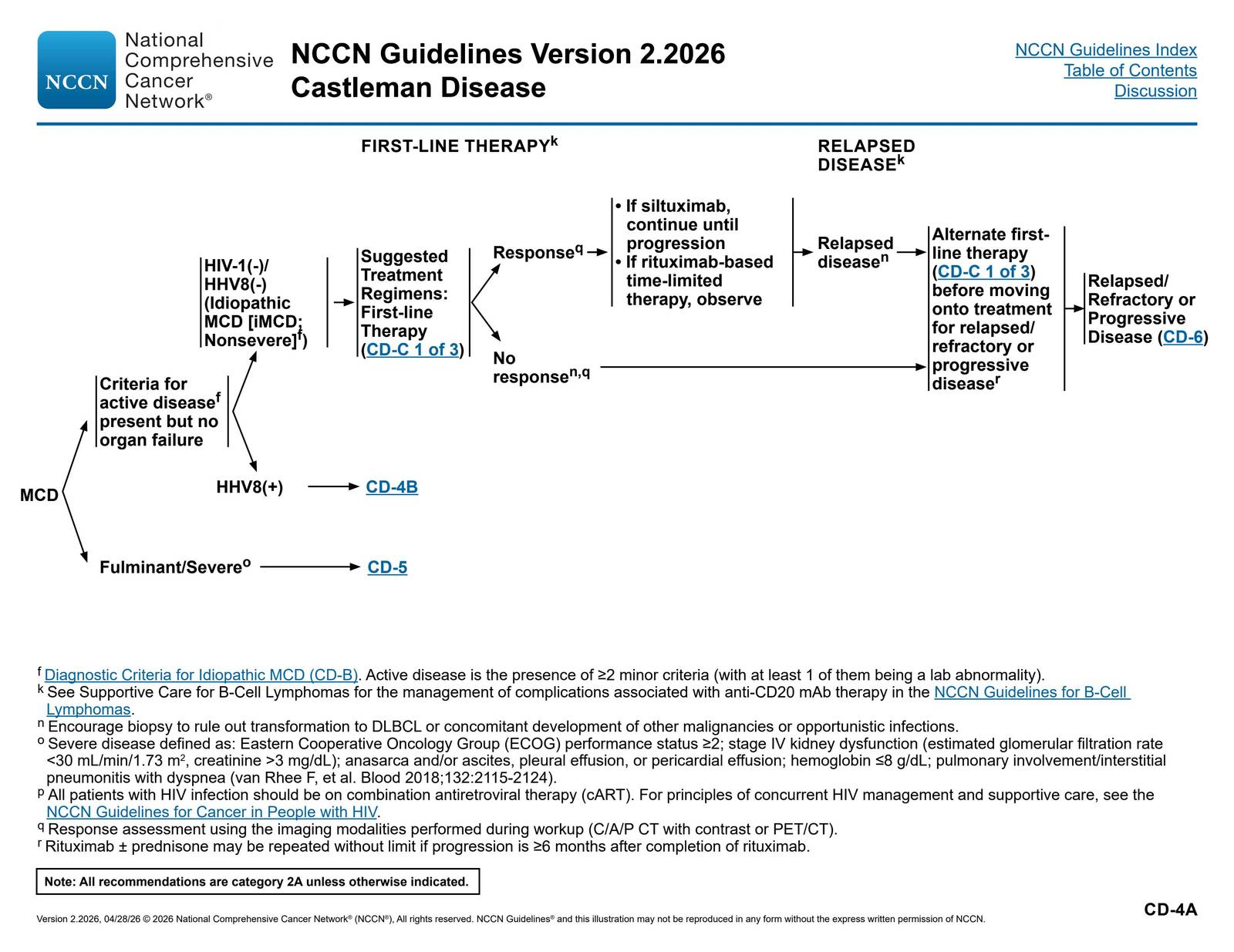
Option (D) is INCORRECT because corticosteroid monotherapy is not adequate first-line treatment for idiopathic MCD-NOS, non-severe disease. According to the Castleman Disease Collaborative Network (CDCN) consensus treatment guidelines and NCCN guidelines, siltuximab (anti-IL-6 therapy) with or without corticosteroids is the recommended first-line treatment for iMCD-NOS non-severe disease13810[^11].
Corticosteroid monotherapy is associated with only a 3% response rate and is explicitly not recommended in consensus guidelines3. While corticosteroids may provide temporary symptom relief, disease flares are nearly universal upon discontinuation, and durable disease control requires anti-IL-6 directed therapy1310. The NCCN guidelines specifically recommend siltuximab as first-line therapy for nonsevere iMCD, with continuation until progression8.
Real-world data from the ACCELERATE Natural History Registry demonstrated that siltuximab with or without corticosteroids achieved a 52% response rate, whereas corticosteroid monotherapy achieved only a 3% response3. Siltuximab is the only FDA-approved therapy for iMCD and is recommended as standard first-line treatment across all major guidelines110[11][13].
Why the Other Statements Are Correct¶
(A) HHV-8-associated MCD treatment is CORRECT. For HHV-8-associated MCD, rituximab is the standard first-line therapy for mild disease[14][15]. In patients with severe systemic symptoms, organ dysfunction, or cytokine storm, etoposide is added to rituximab to achieve more rapid disease control[14][15]. This B-cell directed approach targets the HHV-8-infected plasmablasts that drive disease pathogenesis.
(B) POEMS-MCD treatment is CORRECT. When MCD occurs in association with POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, skin changes), the disease should be treated as POEMS syndrome with plasma cell-directed therapy[14][15][^16]. Standard myeloma induction regimens are used, with autologous stem cell transplantation (ASCT) considered for consolidation[^16]. In one series, all 9 POEMS-MCD patients treated with first-line ASCT achieved at least partial response, with 7 achieving complete response[^16].
(C) iMCD-TAFRO treatment is CORRECT. iMCD-TAFRO (thrombocytopenia, anasarca, fever, renal dysfunction/reticulin fibrosis, organomegaly) represents the most severe subtype with fulminant cytokine storm16[^13]. Treatment requires parenteral corticosteroids combined with anti-IL-6 therapy (siltuximab or tocilizumab)16[^13]. This aggressive approach is necessary given the life-threatening nature of TAFRO syndrome with rapid onset multiorgan dysfunction.
(E) iMCD-NOS severe disease treatment is CORRECT. For severe iMCD-NOS (defined by ECOG performance status ≥2, severe organ dysfunction, anasarca, or severe cytopenias), if anti-IL-6 therapy is unavailable or fails to achieve adequate response, escalation to combination chemotherapy with rituximab-CHOP or rituximab-CVP is recommended15610. This cytotoxic approach nonspecifically eliminates hyperinflammatory cells in patients with progressive organ dysfunction refractory to targeted therapy.
詳解 · 中文翻譯¶
不正確陳述的分析¶
選項 (D) 不正確,因為皮質類固醇單藥治療對於特發性 MCD-NOS 非嚴重疾病來說 不是 充分的一線治療。根據 Castleman 疾病合作網絡(CDCN)共識治療指南和 NCCN 指南,siltuximab(抗 IL-6 治療)伴或不伴皮質類固醇是推薦的 iMCD-NOS 非嚴重疾病的一線治療13810[^11]。
皮質類固醇單藥治療與僅 3% 的反應率 相關聯,在共識指南中明確 不推薦3。雖然皮質類固醇可能提供臨時症狀緩解,但停用時幾乎普遍發生疾病復發,耐久疾病控制需要抗 IL-6 導向治療1310。NCCN 指南特別推薦 siltuximab 作為非嚴重 iMCD 的一線治療,持續至進展8。
真實世界數據來自 ACCELERATE 自然史登記顯示 siltuximab 伴或不伴皮質類固醇達到 52% 反應率,而皮質類固醇單藥治療僅達到 3% 反應3。Siltuximab 是 iMCD 的唯一 FDA 批准的治療,在所有主要指南中被推薦為標準一線治療110[11][13]。
其他陳述為何正確¶
(A) HHV-8 相關 MCD 治療正確。 對於 HHV-8 相關 MCD,rituximab 是輕度疾病的標準一線治療[14][15]。在具有嚴重全身症狀、器官功能障礙或細胞激素風暴的患者中,etoposide 加入 rituximab 以達成更快速的疾病控制[14][15]。此 B 細胞導向方法靶向驅動疾病病理生成的 HHV-8 感染血漿細胞。
(B) POEMS-MCD 治療正確。 當 MCD 伴隨 POEMS 症候群(多神經病、器官腫大、內分泌病、單克隆蛋白、皮膚改變)發生時,疾病應作為 具有血漿細胞導向治療的 POEMS 症候群 被治療[14][15][16]。使用標準骨髓瘤誘導方案,考慮以自體幹細胞移植(ASCT)進行鞏固[16]。在一個系列中,所有 9 例用一線 ASCT 治療的 POEMS-MCD 患者達到至少部分反應,7 人達到完全反應[^16]。
(C) iMCD-TAFRO 治療正確。 iMCD-TAFRO(血小板減少症、全身浮腫、發熱、腎功能障礙/網狀纖維化、器官腫大)代表最嚴重的亞型,伴隨劇烈細胞激素風暴16[^13]。治療需要 靜脈皮質類固醇與抗 IL-6 治療(siltuximab 或 tocilizumab)組合16[^13]。鑑於 TAFRO 症候群危及生命的性質及快速發作多器官功能障礙,此侵襲性方法是必要的。
(E) iMCD-NOS 嚴重疾病治療正確。 對於嚴重 iMCD-NOS(由 ECOG 表現狀態 ≥2、嚴重器官功能障礙、全身浮腫或嚴重細胞減少症定義),如果 抗 IL-6 治療不可用或未能達成充分反應,升級至與 rituximab-CHOP 或 rituximab-CVP 的組合化療 被推薦15610。此細胞毒性方法非特異性地消除對靶向治療有難治性進行性器官功能障礙患者中的高炎症細胞。
參考文獻 (AMA)¶
-
Chen LYC, Zhang L, Fajgenbaum DC. Expert Perspective: Diagnosis and Treatment of Castleman Disease. Arthritis & Rheumatology (Hoboken, N.J.). 2026;78(1):12-25. doi:10.1002/art.43269. PMID:40457814. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Pierson SK, Lim MS, Srkalovic G, et al. Treatment Consistent With Idiopathic Multicentric Castleman Disease Guidelines Is Associated With Improved Outcomes. Blood Advances. 2023;7(21):6652-6664. doi:10.1182/bloodadvances.2023010745. PMID:37656441. ↩
-
National Comprehensive Cancer Network. Castleman Disease. https://www.nccn.org/professionals/physician_gls/pdf/castleman.pdf#page=9. ↩↩↩↩↩↩↩↩
-
Fajgenbaum DC. Novel Insights and Therapeutic Approaches in Idiopathic Multicentric Castleman Disease. Blood. 2018;132(22):2323-2330. doi:10.1182/blood-2018-05-848671. PMID:30487129. ↩
-
Pelliccia S, Di Rocco A, Palumbo G, et al. Siltuximab as a First-Line Therapy for Idiopathic Multicentric Castleman Disease: A Retrospective Analysis Based on the SiMuLa Study of the Italian Regional Network. Frontiers in Oncology. 2026;16:1762473. doi:10.3389/fonc.2026.1762473. PMID:41777649. ↩↩
-
Carbone A, Borok M, Damania B, et al. Castleman Disease. Nature Reviews. Disease Primers. 2021;7(1):84. doi:10.1038/s41572-021-00317-7. PMID:34824298. ↩↩↩↩↩↩
-
Dispenzieri A, Fajgenbaum DC. Overview of Castleman Disease. Blood. 2020;135(16):1353-1364. doi:10.1182/blood.2019000931. PMID:32106302. ↩
-
Abdallah NH, Habermann T, Buadi FK, et al. Multicentric Castleman Disease: A Single Center Experience of Treatment With a Focus on Autologous Stem Cell Transplantation. American Journal of Hematology. 2022;97(4):401-410. doi:10.1002/ajh.26466. PMID:35015310. ↩↩↩↩
-
Zhang L, Ge JY, Li SY, et al. Idiopathic Multicentric Castleman Disease-Tafro: A Potentially Curable Disease?. American Journal of Hematology. 2026;101(3):447-455. doi:10.1002/ajh.70199. PMID:41518092. ↩
-
Fajgenbaum DC, June CH. Cytokine Storm. The New England Journal of Medicine. 2020;383(23):2255-2273. doi:10.1056/NEJMra2026131. PMID:33264547. ↩↩↩↩↩↩↩↩
Figures¶