Q1. About the first-line treatment of follicular lymphoma, which of the below descriptions are wrong?¶
- (A) Watch and wait is suggested in asymptomatic FL patients.
- (B) Obinutuzumab-chemotherapy produces better outcome than rituximab-based immunochemotherapy.
- (C) Bendamustine-based immunotherapy is recommended in elderly patients because bendamustine has less myeloid suppression and lymphotoxicity.
- (D) Maintenance therapy with rituximab or Obinutuzumab is indicated in FL after induction immunochemotherapy.
- (E) Clinical outcomes among patients with FL of grades 1, 2, and 3A seem not to be significantly different.
點此顯示正解
(C) Bendamustine-based immunotherapy is recommended in elderly patients because bendamustine has less myeloid suppression and lymphotoxicity.
詳解¶
Analysis of Board Question¶
1. Why (C) is the INCORRECT statement:
Option (C) states that bendamustine-based immunotherapy is recommended in elderly patients because bendamustine has less myeloid suppression and lymphotoxicity. This is factually wrong. Bendamustine actually causes significant myelosuppression and prolonged lymphotoxicity:
- Bendamustine causes severe lymphopenia (99% of patients experience decreased lymphocytes, with 94% having Grade 3/4 lymphopenia)[^8]
- It causes significant neutropenia (86% of patients, with 60% Grade 3/4)[^8]
- Bendamustine leads to higher rates of prolonged and unresolved lymphocytopenia compared to CHOP/CVP, with many patients not recovering lymphocyte counts even 3 years after treatment[^7]
- It causes greater incidence of late-onset neutropenia compared to CHOP/CVP[^7]
While bendamustine is indeed a preferred first-line regimen for follicular lymphoma (including in elderly patients)2, the rationale is not reduced myelosuppression or lymphotoxicity. The actual advantages include efficacy comparable to CHOP with potentially less cardiotoxicity (no anthracycline) and convenience (2-day infusion schedule). The statement's premise about "less myeloid suppression and lymphotoxicity" is the opposite of reality.
2. Why the other options are TRUE:
(A) Watch and wait is suggested in asymptomatic FL patients — TRUE
This is standard practice for low tumor burden, asymptomatic follicular lymphoma. Treatment should only be initiated based on presence of B-symptoms, hematopoietic impairment, bulky disease, vital organ compression, ascites, pleural effusion, or rapid progression3. The NCCN guidelines specifically recommend observation as an option for asymptomatic patients with low tumor burden2.
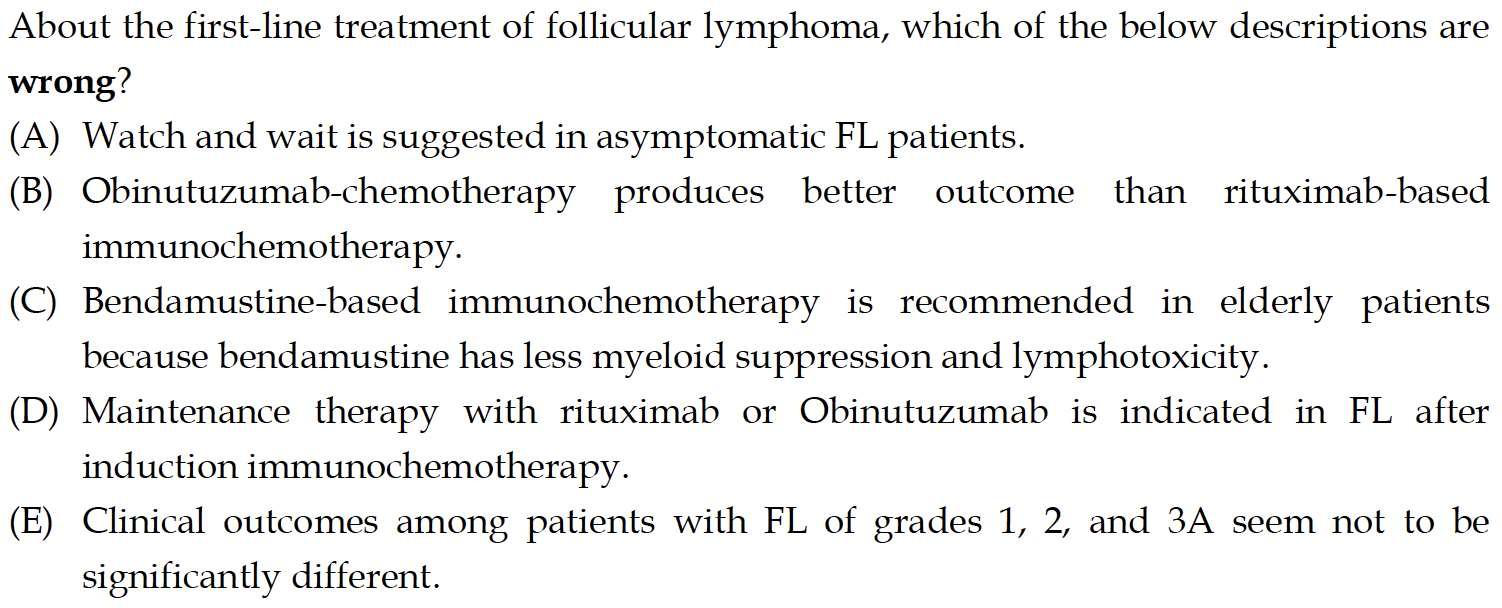
(B) Obinutuzumab-chemotherapy produces better outcome than rituximab-based immunochemotherapy — TRUE
The landmark GALLIUM trial demonstrated that obinutuzumab-based chemotherapy resulted in significantly longer progression-free survival compared to rituximab-based therapy (3-year PFS: 80.0% vs 73.3%; HR 0.66, 95% CI 0.51-0.85, p=0.001)4. Network meta-analysis confirmed obinutuzumab had the highest effect sizes for PFS (HR 0.43, 95% CI 0.22-0.79)5.
(D) Maintenance therapy with rituximab or obinutuzumab is indicated in FL after induction immunochemotherapy — TRUE
Maintenance therapy with rituximab (every 8-12 weeks for 2 years) or obinutuzumab (every 8 weeks for 12 doses) improves progression-free survival after induction immunochemotherapy12. The NCCN guidelines list both as preferred options for extended therapy following chemoimmunotherapy, with rituximab maintenance being Category 1 evidence2.
(E) Clinical outcomes among patients with FL of grades 1, 2, and 3A seem not to be significantly different — TRUE
Follicular lymphoma grades 1, 2, and 3A are treated similarly and have comparable clinical outcomes. They are all considered indolent lymphomas and managed with the same treatment algorithms. Grade 3B is treated differently (like diffuse large B-cell lymphoma), but grades 1, 2, and 3A are grouped together in clinical practice and guidelines2.
詳解 · 中文翻譯¶
板考分析¶
1. 為什麼 (C) 是不正確的敘述:
選項 (C) 陳述 bendamustine 基礎免疫療法在老年患者中被推薦因為 bendamustine 有較少的骨髓抑制和淋巴毒性。這是事實上錯誤的。Bendamustine 實際上引起顯著骨髓抑制和延長的淋巴毒性:
- Bendamustine 引起嚴重淋巴細胞減少症(99% 的患者經歷淋巴細胞減少,94% 為 3/4 級)[^8]
- 它引起顯著中性粒細胞減少症(86% 的患者,60% 為 3/4 級)[^8]
- Bendamustine 導致比 CHOP/CVP 更高的延長和未解決的淋巴細胞減少症率,許多患者即使在治療後 3 年仍未恢復淋巴細胞計數[^7]
- 它導致比 CHOP/CVP 更大的遲發性中性粒細胞減少症發生率[^7]
雖然 bendamustine 確實是濾泡淋巴瘤的首選一線方案(包括在老年患者中)2,但原理不是骨髓抑制或淋巴毒性減少。實際的優勢包括與 CHOP 相當的療效,可能具有較少的心臟毒性(無蒽環類)和便利(2 天輸注時間表)。該敘述的「較少骨髓抑制和淋巴毒性」的前提與現實相反。
2. 為什麼其他選項是正確的:
(A) 無症狀 FL 患者建議觀察和等待 — 正確
這是低腫瘤負擔、無症狀濾泡淋巴瘤的標準實踐。治療應僅在存在 B 症狀、造血損害、大塊疾病、重要器官壓迫、腹水、胸腔積液或快速進展時進行3。NCCN 指南特別推薦對低腫瘤負擔的無症狀患者進行觀察作為一項選擇2。
(B) Obinutuzumab 化療比利妥昔單抗基礎免疫化療產生更好結果 — 正確
標誌性 GALLIUM 試驗證明 obinutuzumab 基礎化療與利妥昔單抗基礎治療相比導致顯著更長的無進展生存期(3 年 PFS:80.0% vs 73.3%;HR 0.66,95% CI 0.51-0.85,p=0.001)4。網路統合分析確認 obinutuzumab 在 PFS 中具有最高的效應大小(HR 0.43,95% CI 0.22-0.79)5。
(D) 在歸納免疫化療後用利妥昔單抗或 obinutuzumab 進行維持治療 — 正確
用利妥昔單抗(每 8-12 週 2 年)或 obinutuzumab(每 8 週 12 次劑量)進行維持治療改善歸納免疫化療後的無進展生存期12。NCCN 指南將兩者列為化療免疫治療後延長治療的首選選項,利妥昔單抗維持治療為 1 類證據2。
(E) 1、2 和 3A 級 FL 患者的臨床結果似乎沒有顯著不同 — 正確
濾泡淋巴瘤 1、2 和 3A 級的治療類似並具有相當的臨床結果。它們都被認為是惰性淋巴瘤,並用相同的治療算法進行管理。3B 級的治療方式不同(如瀰漫大 B 細胞淋巴瘤),但 1、2 和 3A 級在臨床實踐和指南中被組合在一起2。
參考文獻 (AMA)¶
-
Food and Drug Administration. Bendamustine Hydrochloride. 2025. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=085dd54c-4212-d879-afef-ee52732a48c0. ↩↩
-
Baek GT, Mathis NJ, Perissinotti AJ, et al. Late-Onset Complications With Bendamustine Versus CHOP or CVP Based Chemoimmunotherapy in Indolent Non-Hodgkin's Lymphoma. Leukemia & Lymphoma. 2021;62(13):3138-3146. doi:10.1080/10428194.2021.1953014. PMID:34263702. ↩↩↩↩↩↩↩↩↩↩
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=22. ↩↩
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩
-
Marcus R, Davies A, Ando K, et al. Obinutuzumab for the First-Line Treatment of Follicular Lymphoma. The New England Journal of Medicine. 2017;377(14):1331-1344. doi:10.1056/NEJMoa1614598. PMID:28976863. ↩↩
-
Chu Y, Liu Y, Yu Z, et al. Maintenance and Consolidation Strategies for Patients With Untreated Advanced Follicular Lymphoma: A Systematic Review and Network Meta-Analysis of Randomized Trials. Cancer. 2024;130(7):1072-1082. doi:10.1002/cncr.35137. PMID:38041532. ↩
Slide annotations
Myelosuppression including lymphopenia occurs relatively frequently after therapy with bendamustine. It is mostly CD4 + T cell counts that are suppressed.
Figures¶