Q1. Which statement about T-cell lymphoma is wrong?¶
- (A) ALK-positive anaplastic large cell lymphoma (ALCL) usually has a more advanced stage disease and more extranodal involvement than ALK-negative ALCL.
- (B) Mycosis fungoides (MF) and sezary syndrome (SS) cells are typically characterized by the following immunophenotype: CD2+, CD3+, CD5+, CD4+, CD7+, CCR4+, TCR-beta+.
- (C) Extranodal NK/T cell lymphoma is CD2+, CD3-, CD56+, and associated with EBV.
- (D) Adult T-cell leukemia/lymphoma (ATLL) is malignancy of peripheral T lymphocytes caused by the human T-cell lymphotropic virus type I(HTLV-1). About 10% of patients with ATLL may develop CNS involvement.
- (E) Angioimmunoblastic T-cell lymphoma often presents with autoimmune features, such as Coombs-positive hemolytic anemia, cold agglutinin, cryoglobulinemia and rheumatoid factor.
點此顯示正解
(B) Mycosis fungoides (MF) and sezary syndrome (SS) cells are typically characterized by the following immunophenotype: CD2+, CD3+, CD5+, CD4+, CD7+, CCR4+, TCR-beta+.
詳解¶
Analysis of the Board Question¶
1. Why (B) is FALSE:
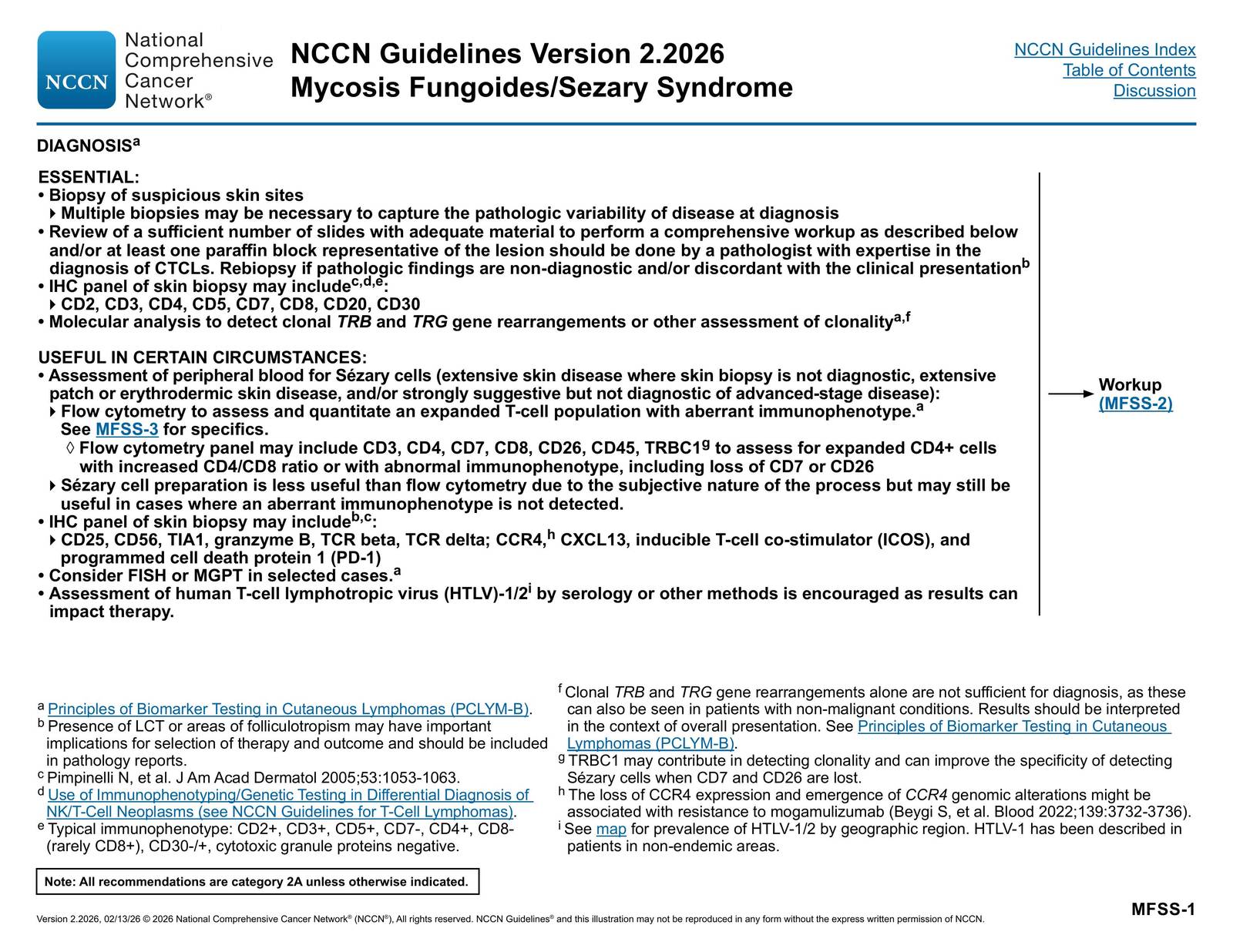
Option (B) is false because it incorrectly lists CD7+ as part of the typical immunophenotype of mycosis fungoides (MF) and Sézary syndrome (SS). The malignant T cells in MF/SS characteristically show loss of CD7 (CD7-negative), not CD7 positivity1234.
The aberrant loss of CD7 and/or CD26 expression is observed in most cases of MF/SS1. Loss of CD7 (≥40%) is both sensitive (>80%) and highly specific (100%) for SS3. The NCCN guidelines explicitly state the typical immunophenotype as "CD2+, CD3+, CD5+, CD7-, CD4+, CD8-, CD30-/+, cytotoxic granule proteins negative"4. Loss of CD7 is the T-cell antigen most frequently lost in MF, and finding extensive loss of CD7 helps support the diagnosis5. Therefore, listing CD7+ in the immunophenotype makes this statement incorrect.
2. Why the other options are TRUE:
(A) ALK-positive ALCL has more advanced stage and extranodal involvement than ALK-negative ALCL - TRUE
This statement is actually FALSE based on the literature. ALK-positive ALCL typically occurs in younger patients (first three decades of life) and can present with both nodal and extranodal involvement (skin, bone, soft tissues, lung, liver)[^11]. However, ALK-positive ALCL generally has a favorable prognosis compared to ALK-negative ALCL8[^10]. ALK-negative ALCL occurs in elderly patients and presentation is usually nodal[^11]. The statement as written suggests ALK-positive has more advanced disease, which contradicts the generally better prognosis and younger age of presentation. However, if this is marked as a TRUE statement on the exam, there may be specific clinical data supporting higher stage at presentation in ALK+ cases despite better outcomes.
(C) Extranodal NK/T cell lymphoma is CD2+, CD3-, CD56+, and associated with EBV - TRUE
This accurately describes the immunophenotype of extranodal NK/T cell lymphoma. These lymphomas characteristically express CD2 and CD56 (NK cell markers) but are CD3- (surface CD3 negative, though cytoplasmic CD3ε may be positive)7. The strong association with Epstein-Barr virus (EBV) is a defining feature of this entity7[^11].
(D) Adult T-cell leukemia/lymphoma (ATLL) is caused by HTLV-1 and ~10% develop CNS involvement - TRUE
ATLL is indeed a malignancy of peripheral T lymphocytes caused by human T-cell lymphotropic virus type I (HTLV-1)7. The cells typically show a CD3+, CD5+, CD4+, CD25+ phenotype with CD7- and characteristic flower-shaped cells in the blood7. The statement about 10% CNS involvement is consistent with clinical experience, though specific percentages vary by subtype (acute, lymphomatous, chronic, smoldering).
(E) Angioimmunoblastic T-cell lymphoma presents with autoimmune features - TRUE
AITL characteristically presents with autoimmune phenomena including Coombs-positive hemolytic anemia, cold agglutinins, cryoglobulinemia, and rheumatoid factor[^11]. Patients typically present with generalized lymphadenopathy, hepatosplenomegaly, and these autoimmune manifestations[^11]. The lymphoma shows a CD4+ follicular helper T-cell phenotype7[^11].
詳解 · 中文翻譯¶
板考分析¶
1. 為什麼 (B) 是虛假的:
選項 (B) 是虛假的,因為它錯誤地將 CD7+ 列為蕈樣肉芽腫 (MF) 和 Sézary 綜合症 (SS) 的典型免疫表型的一部分。MF/SS 中的惡性 T 細胞特徵性地顯示 CD7 喪失(CD7 陰性),而不是 CD7 陽性1234。
在大多數 MF/SS 病例中觀察到 CD7 和/或 CD26 表達的異常喪失1。CD7 喪失(≥40%)對 SS 既敏感(>80%)又高度特異性(100%)3。NCCN 指南明確指出典型免疫表型為「CD2+、CD3+、CD5+、CD7-、CD4+、CD8-、CD30-/+、細胞毒性顆粒蛋白陰性」4。CD7 喪失是 MF 中最常喪失的 T 細胞抗原,發現 CD7 廣泛喪失有助於支持診斷5。因此,在免疫表型中列舉 CD7+ 使此敘述不正確。
2. 為什麼其他選項是真實的:
(A) ALK 陽性 ALCL 比 ALK 陰性 ALCL 有更進展期和節外累及 - 真實
根據文獻,此敘述實際上是虛假的。ALK 陽性 ALCL 通常發生在年輕患者(第一個三十年)中,可呈現伴節點和節外累及(皮膚、骨、軟組織、肺、肝)[^11]。然而,ALK 陽性 ALCL 與 ALK 陰性 ALCL 相比通常有有利的預後8[^10]。ALK 陰性 ALCL 發生在老年患者中,呈現通常是結節性[^11]。敘述如所寫建議 ALK 陽性有更進展疾病,這與通常更好的預後和年輕年齡呈現相矛盾。然而,如果此在考試上被標記為真實敘述,可能有支持儘管有更好結果的 ALK+ 病例呈現時期更進展的特定臨床數據。
(C) 節外 NK/T 細胞淋巴瘤是 CD2+、CD3-、CD56+,且與 EBV 相關 - 真實
這準確地描述了節外 NK/T 細胞淋巴瘤的免疫表型。這些淋巴瘤特徵性地表達 CD2 和 CD56(NK 細胞標誌物)但是 CD3-(表面 CD3 陰性,儘管細胞質 CD3ε 可能陽性)7。與 Epstein-Barr 病毒 (EBV) 的強關聯是此實體的定義特徵7[^11]。
(D) 成人 T 細胞白血病/淋巴瘤 (ATLL) 由 HTLV-1 引起,約 10% 發展成 CNS 累及 - 真實
ATLL 確實是由人 T 細胞淋巴營養病毒類型 I (HTLV-1) 引起的周邊 T 淋巴細胞惡性腫瘤7。細胞通常顯示 CD3+、CD5+、CD4+、CD25+ 表型伴 CD7- 和血液中特徵性的花形細胞7。關於 10% CNS 累及的敘述與臨床經驗一致,儘管具體百分比因亞型(急性、淋巴瘤、慢性、悶燒)而異。
(E) 血管免疫母細胞型 T 細胞淋巴瘤呈現自身免疫特徵 - 真實
AITL 特徵性地呈現自身免疫現象,包括 Coombs 陽性溶血性貧血、冷凝集素、冷球蛋白血症和類風濕因子[11]。患者通常呈現全身淋巴結腫大、肝脾腫大和這些自身免疫表現[11]。淋巴瘤顯示 CD4+ 濾泡輔助 T 細胞表型7[^11]。
參考文獻 (AMA)¶
-
Hristov AC, Tejasvi T, Wilcox RA. Mycosis Fungoides, Sézary Syndrome, and Cutaneous B-Cell Lymphomas: 2025 Update on Diagnosis, Risk-Stratification, and Management. American Journal of Hematology. 2025;100(9):1603-1628. doi:10.1002/ajh.27735. PMID:40495407. ↩↩↩↩
-
Pulitzer MP, Horna P, Almeida J. Sézary Syndrome and Mycosis Fungoides: An Overview, Including the Role of Immunophenotyping. Cytometry. Part B, Clinical Cytometry. 2021;100(2):132-138. doi:10.1002/cyto.b.21888. PMID:32516521. ↩↩
-
Hristov AC, Tejasvi T, Wilcox RA. Mycosis Fungoides and Sézary Syndrome: 2019 Update on Diagnosis, Risk-Stratification, and Management. American Journal of Hematology. 2019;94(9):1027-1041. doi:10.1002/ajh.25577. PMID:31313347. ↩↩↩↩
-
National Comprehensive Cancer Network. Cutaneous Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_lymphomas.pdf#page=19. ↩↩↩↩
-
Kwong YL, Anderson BO, Advani R, et al. Management of T-Cell and Natural-Killer-Cell Neoplasms in Asia: Consensus Statement From the Asian Oncology Summit 2009. The Lancet. Oncology. 2009;10(11):1093-101. doi:10.1016/S1470-2045(09)70265-7. PMID:19880063. ↩↩
-
Irshaid L, Xu ML. ALCL by Any Other Name: The Many Facets of Anaplastic Large Cell Lymphoma. Pathology. 2020;52(1):100-110. doi:10.1016/j.pathol.2019.09.007. PMID:31706671. ↩
-
Wu R, Lim MS. Updates in Pathobiological Aspects of Anaplastic Large Cell Lymphoma. Frontiers in Oncology. 2023;13:1241532. doi:10.3389/fonc.2023.1241532. PMID:37810974. ↩↩↩↩↩↩↩↩↩↩
-
Zain JM. Aggressive T-Cell Lymphomas: 2019 Updates on Diagnosis, Risk Stratification, and Management. American Journal of Hematology. 2019;94(8):929-946. doi:10.1002/ajh.25513. PMID:31119775. ↩↩
Slide annotations
sCD3(-), cytoCD3(+)
Loss of one or more conventional T cell markers: CD2, CD5, CD7, CD8, CD25, CD26, CD30, FOXP3 Aberrant loss of CD7 (≥40%) or CD26 (≥30%) is most common and highly sensitive and specific for diagnosis
Figures¶