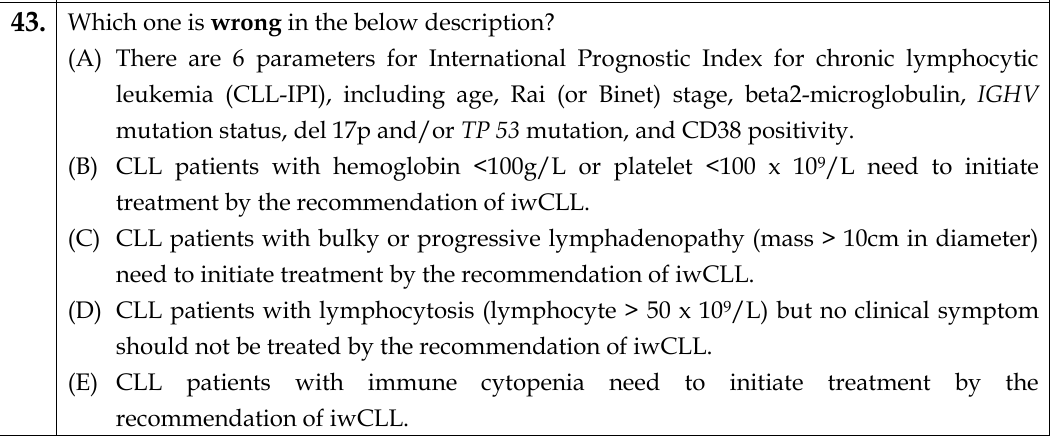
Q43. Which one is wrong in the below description?¶
- (A) There are 6 parameters for International Prognostic Index for chronic lymphocytic leukemia (CLL-IPI), including age, Rai (or Binet) stage, beta2-microglobulin, IGHV mutation status, del 17p and/or TP 53 mutation, and CD38 positivity.
- (B) CLL patients with hemoglobin <100g/L or platelet <100 x 10^9/L need to initiate treatment by the recommendation of iwCLL.
- (C) CLL patients with bulky or progressive lymphadenopathy (mass > 10cm in diameter) need to initiate treatment by the recommendation of iwCLL.
- (D) CLL patients with lymphocytosis (lymphocyte > 50 x 10^9/L) but no clinical symptom should not be treated by the recommendation of iwCLL.
- (E) CLL patients with immune cytopenia need to initiate treatment by the recommendation of iwCLL.
點此顯示正解
(A) There are 6 parameters for International Prognostic Index for chronic lymphocytic leukemia (CLL-IPI), including age, Rai (or Binet) stage, beta2-microglobulin, IGHV mutation status, del 17p and/or TP 53 mutation, and CD38 positivity.
詳解¶
Analysis of Board Question¶
Why (A) is the INCORRECT statement:
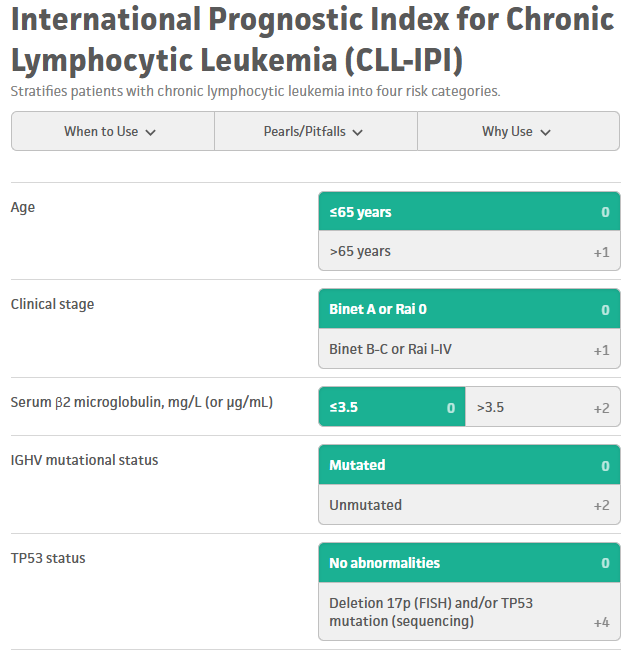
Option (A) states that the CLL-IPI includes 6 parameters, but the CLL-IPI actually contains only 5 parameters. The correct five components are: (1) age >65 years, (2) clinical stage (Rai I-IV or Binet B-C), (3) serum β2-microglobulin >3.5 mg/L, (4) IGHV mutational status (unmutated), and (5) TP53 status (del[17p] and/or TP53 mutation)124. CD38 positivity is NOT part of the CLL-IPI—this is the key error that makes option (A) incorrect. While CD38 is a prognostic marker in CLL, it was not included in the final CLL-IPI model derived from the international meta-analysis1.
Why the other options are CORRECT:
(B) is correct: The iwCLL guidelines specify that hemoglobin <10 g/dL or platelet count <100 × 10⁹/L are indications for treatment initiation when due to progressive marrow failure from CLL67[10][12]. The question states <100 g/L (equivalent to <10 g/dL) for hemoglobin and <100 × 10⁹/L for platelets, which matches the iwCLL criteria.
(C) is correct: The iwCLL treatment criteria include massive (≥10 cm in longest dimension) or progressive or symptomatic lymphadenopathy as an indication for treatment6[9][14]. This matches the statement about bulky or progressive lymphadenopathy with mass >10 cm in diameter.
(D) is correct: While the iwCLL guidelines technically list progressive lymphocytosis (≥50% increase over 2 months or lymphocyte doubling time <6 months) as a treatment criterion, lymphocytosis alone without other symptoms should not trigger treatment6[^17]. Recent expert opinion emphasizes that this criterion should not be used in isolation, and asymptomatic patients with lymphocytosis alone (even >50 × 10⁹/L) should not be treated6. The statement correctly reflects that lymphocytosis without clinical symptoms should not prompt treatment.
(E) is correct: The iwCLL guidelines explicitly include autoimmune anemia or thrombocytopenia poorly responsive to steroids as an indication for CLL treatment6[9][12]. This is distinct from cytopenias due to marrow failure and represents immune-mediated cytopenia requiring CLL-directed therapy.
詳解 · 中文翻譯¶
為何 (A) 是錯誤陳述:
選項 (A) 指出 CLL-IPI 包含 6 個參數,但 CLL-IPI 實際上只有 5 個參數。正確的五項組成為:(1) 年齡 >65 歲、(2) 臨床分期(Rai I-IV 或 Binet B-C)、(3) 血清 β2-微球蛋白 >3.5 mg/L、(4) IGHV 突變狀態(未發生突變)和 (5) TP53 狀態(del[17p] 和/或 TP53 突變)124。CD38 陽性並非 CLL-IPI 的一部分——這是使選項 (A) 錯誤的關鍵誤導。雖然 CD38 是 CLL 的預後標誌物,但它並未被納入國際薈萃分析衍生的最終 CLL-IPI 模型1。
其他選項為何正確:
(B) 正確: iwCLL 指南規定 血紅素 <10 g/dL 或血小板計數 <100 × 10⁹/L 是當由於 CLL 導致的進行性骨髓衰竭時啟動治療的適應症67[10][12]。題目指出血紅素 <100 g/L(等同於 <10 g/dL)和血小板 <100 × 10⁹/L,符合 iwCLL 標準。
(C) 正確: iwCLL 治療標準包括 巨大(最長徑 ≥10 cm)或進行性或有症狀的淋巴結腫大 作為治療適應症6[9][14]。這符合關於直徑 >10 cm 的腫塊型或進行性淋巴結腫大的陳述。
(D) 正確: 雖然 iwCLL 指南技術上列出進行性淋巴球增多(2 個月內 ≥50% 增長或淋巴球倍增時間 <6 個月)作為治療標準,但 單純淋巴球增多而無其他症狀不應觸發治療6[^17]。近期專家意見強調此標準不應單獨使用,無症狀但單純淋巴球增多的患者(即使 >50 × 10⁹/L)不應接受治療6。該陳述正確地反映無臨床症狀的淋巴球增多不應促發治療。
(E) 正確: iwCLL 指南明確列入 類固醇難以控制的自身免疫溶血或血小板減少症 作為 CLL 治療的適應症6[9][12]。這與骨髓衰竭導致的細胞減少症不同,代表需要 CLL 導向治療的免疫介導細胞減少症。
參考文獻 (AMA)¶
-
International CLL-IPI working group. An International Prognostic Index for Patients With Chronic Lymphocytic Leukaemia (CLL-IPI): A Meta-Analysis of Individual Patient Data. The Lancet. Oncology. 2016;17(6):779-790. doi:10.1016/S1470-2045(16)30029-8. PMID:27185642. ↩↩↩↩
-
Kreuzberger N, Damen JA, Trivella M, et al. Prognostic Models for Newly-Diagnosed Chronic Lymphocytic Leukaemia in Adults: A Systematic Review and Meta-Analysis. The Cochrane Database of Systematic Reviews. 2020;7:CD012022. doi:10.1002/14651858.CD012022.pub2. PMID:32735048. ↩↩
-
Jain N, Wierda WG, O'Brien S. Chronic Lymphocytic Leukaemia. Lancet (London, England). 2024;404(10453):694-706. doi:10.1016/S0140-6736(24)00595-6. PMID:39068951. ↩
-
Hallek M. Chronic Lymphocytic Leukemia: 2025 Update on the Epidemiology, Pathogenesis, Diagnosis, and Therapy. American Journal of Hematology. 2025;100(3):450-480. doi:10.1002/ajh.27546. PMID:39871707. ↩↩
-
Hallek M, Al-Sawaf O. Chronic Lymphocytic Leukemia: 2022 Update on Diagnostic and Therapeutic Procedures. American Journal of Hematology. 2021;96(12):1679-1705. doi:10.1002/ajh.26367. PMID:34625994. ↩
-
Hallek M. Chronic Lymphocytic Leukemia: 2020 Update on Diagnosis, Risk Stratification and Treatment. American Journal of Hematology. 2019;94(11):1266-1287. doi:10.1002/ajh.25595. PMID:31364186. ↩↩↩↩↩↩↩↩↩↩
-
Hallek M. Chronic Lymphocytic Leukemia: 2017 Update on Diagnosis, Risk Stratification, and Treatment. American Journal of Hematology. 2017;92(9):946-965. doi:10.1002/ajh.24826. PMID:28782884. ↩↩
-
Shadman M. Diagnosis and Treatment of Chronic Lymphocytic Leukemia: A Review. Jama. 2023;329(11):918-932. doi:10.1001/jama.2023.1946. PMID:36943212. ↩
Figures¶