Q1. 有關治療與診斷 Post-transplant lymphoproliferative disease (PTLD),下列敘述何者不正確?¶
- (A) 多數與 EBV 感染有關,所以抗病毒藥物有很好的療效。
- (B) 常合併淋巴腺腫大、發燒、肝功能異常。
- (C) Monomorphic PTLD 比 polymorphic PTLD 預後差。
- (D) EBV-PTLD 可以發生於非血液科的疾病及腫瘤。
- (E) 低強度化療合併 anti-CD20 單株抗體是標準治療。
點此顯示正解
(A) 多數與 EBV 感染有關,所以抗病毒藥物有很好的療效。
詳解¶
Analysis of Taiwan Hematology Board Exam Question on PTLD¶
1. Why Option (A) is FALSE¶
Antiviral drugs have no efficacy as monotherapy in established PTLD despite the EBV association. The NEJM review explicitly states that antiviral therapy has "no efficacy as monotherapy (absence of viral thymidine kinase expression in EBV-positive PTLD)"1. The American Society of Transplantation guidelines confirm that "there is no evidence to support the use of antiviral agents in the absence of other interventions such as decreasing immunosuppression or anti-CD20 therapy"2.
The mechanistic explanation is that EBV in PTLD lesions exists predominantly in a latent state, not the lytic (replicative) phase. Acyclovir and ganciclovir require viral thymidine kinase—expressed only during lytic replication—to be phosphorylated into their active forms12. Without lytic infection, these antivirals cannot be activated and therefore lack therapeutic effect. While experimental approaches using histone deacetylase inhibitors (e.g., arginine butyrate) to induce lytic EBV replication combined with ganciclovir showed some promise, these agents are no longer clinically available12.
2. Why the Other Options are TRUE¶
Option (B): Clinical presentation with lymphadenopathy, fever, and abnormal liver function
PTLD commonly presents with lymphadenopathy and constitutional symptoms including fever. Liver involvement is frequent, manifesting as abnormal liver function tests. The heterogeneous nature of PTLD allows for diverse presentations ranging from localized lymphadenopathy to disseminated disease with organ involvement456.
Option (C): Monomorphic PTLD has worse prognosis than polymorphic PTLD
Monomorphic PTLD carries a worse prognosis compared to polymorphic subtypes. The NEJM review demonstrates this through treatment algorithms: polymorphic PTLD often responds to reduction of immunosuppression (RIS) alone with high response rates, whereas monomorphic PTLD—particularly non-DLBCL subtypes—requires more aggressive therapy and is "not indicated as sole up-front therapy" with RIS alone1. The NCCN guidelines similarly stratify treatment intensity by histology, with monomorphic B-cell PTLD requiring rituximab and/or chemoimmunotherapy upfront rather than RIS alone3[^8]. Outcomes for high-risk patients who fail frontline therapy "remain dismal"56.
Option (D): EBV-PTLD occurs beyond hematologic transplant settings
PTLD occurs after both solid organ transplant (SOT) and hematopoietic stem cell transplant (HSCT), as well as in other immunosuppressed states. The literature consistently describes PTLD as a complication of "solid organ transplant and hematopoietic stem cell transplant"456. The American Society of Transplantation guidelines specifically address "solid organ transplantation"2, and treatment approaches differ between SOT-PTLD and HSCT-PTLD, with RIS being more effective in SOT than HSCT1[^9].
Option (E): Low-intensity chemotherapy combined with anti-CD20 antibody is standard treatment
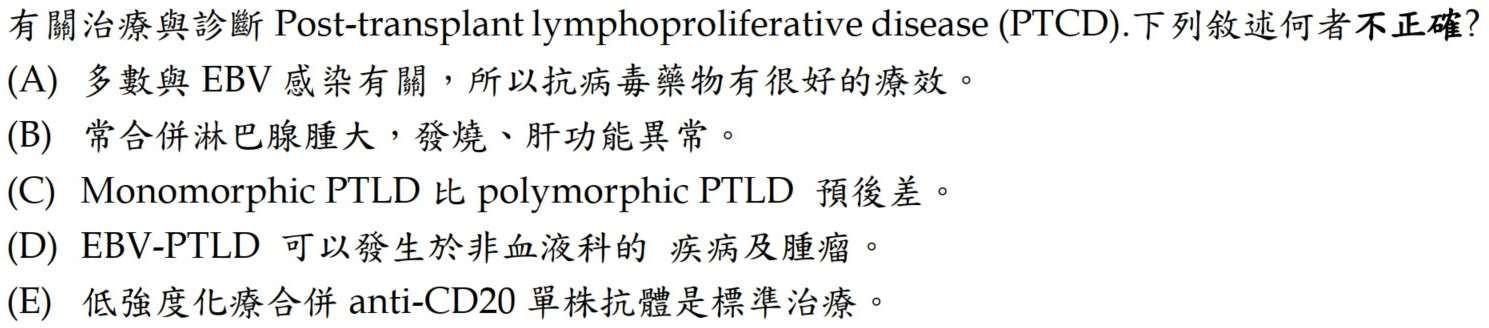
The risk-stratified sequential approach using rituximab (anti-CD20) with or without chemotherapy represents the standard treatment paradigm for monomorphic and polymorphic B-cell PTLD456[^9]. The NCCN guidelines recommend sequential chemoimmunotherapy starting with rituximab, followed by CHOP-R if PET-positive, or concurrent chemoimmunotherapy with CHOP-R or reduced-intensity regimens (CEOP-R, CVP-R, GCVP-R) for frail patients[^10]. This approach allows approximately 25% of patients to avoid chemotherapy entirely56. The following NCCN treatment algorithm illustrates this stepwise strategy:
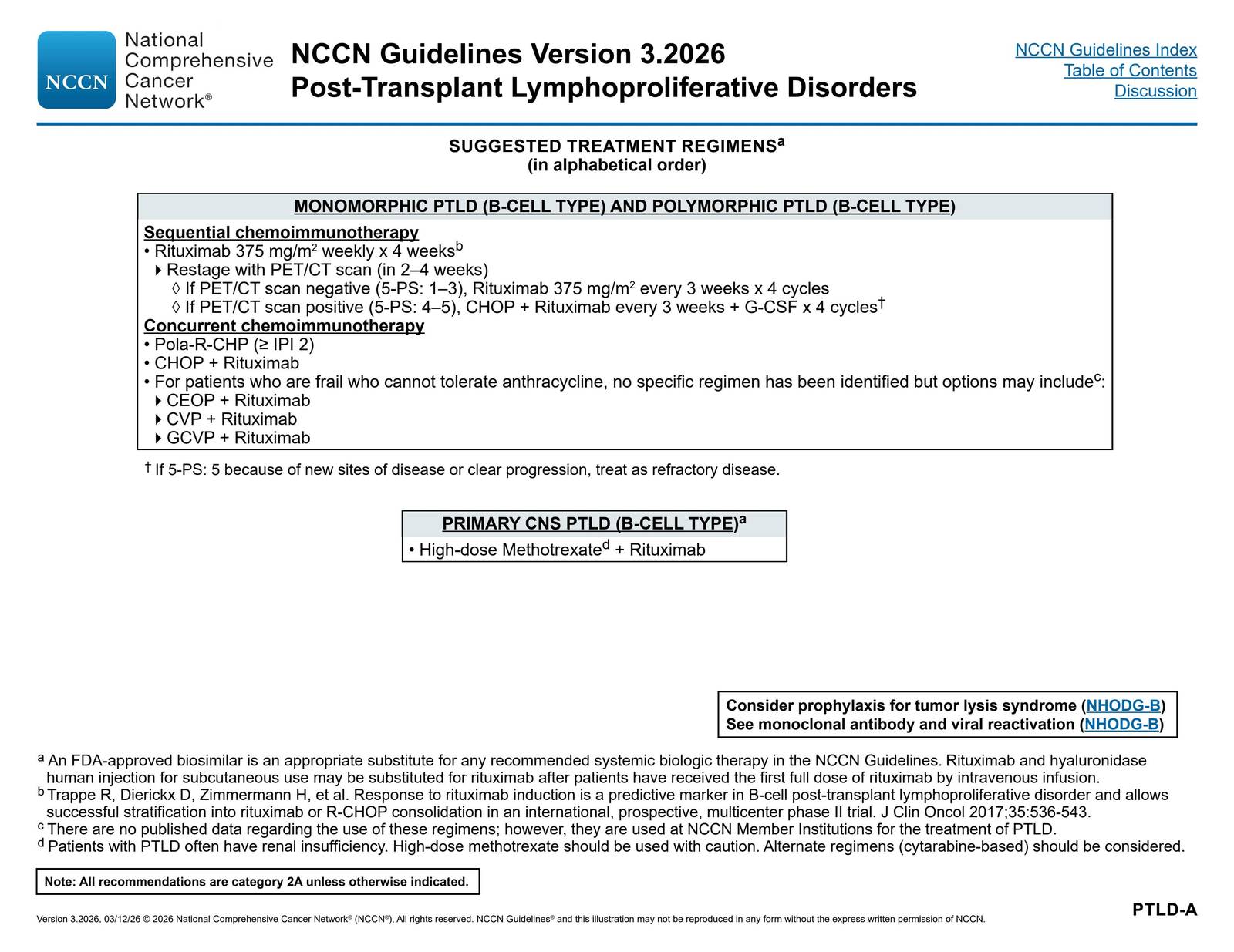
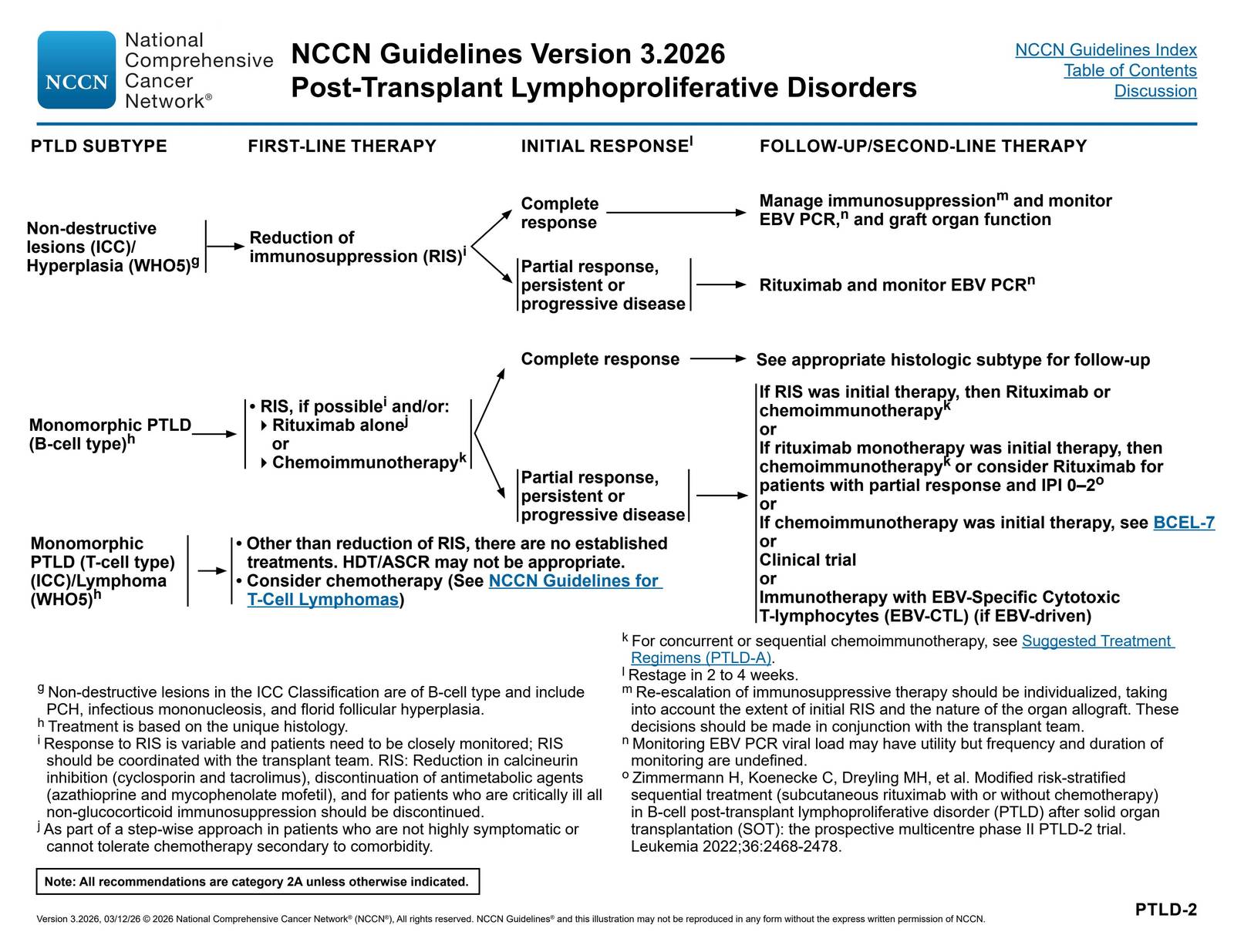
The treatment spectrum from immunosuppression reduction through rituximab to chemotherapy is further illustrated here:

The NCCN first-line treatment algorithm by PTLD subtype:
詳解 · 中文翻譯¶
台灣血液委員會試題分析—PTLD 的治療與診斷¶
1. 為何選項 (A) 錯誤¶
抗病毒藥物在已確立的 PTLD 中不具單獨療效,儘管與 EBV 相關。NEJM 文獻評論明確指出抗病毒治療「不具單獨療效(EBV 陽性 PTLD 中缺乏病毒胸腺苷激酶表達)」1。美國移植學會指南確認「在沒有其他介入措施(如降低免疫抑制或 anti-CD20 治療)的情況下,不存在支持使用抗病毒藥物的證據」2。
機制學解釋是 PTLD 病變中的 EBV 主要處於 潛伏狀態,而非溶解(複製)期。Acyclovir 和 ganciclovir 需要病毒胸腺苷激酶—僅在溶解複製期表達—才能被磷酸化成其活躍形式12。在沒有溶解感染的情況下,這些抗病毒藥物無法被激活,因此缺乏治療效果。雖然使用組蛋白去乙醯酶抑制劑(例如精氨酸丁酸鹽)誘導溶解性 EBV 複製並合併 ganciclovir 的實驗性方法顯示一些前景,但這些藥物已不再臨床可用12。
2. 為何其他選項正確¶
選項 (B):臨床表現為淋巴腺腫大、發燒及異常肝功能
PTLD 常表現為 淋巴腺腫大及全身症狀,包括發燒。肝臟受累常見,表現為肝功能檢驗異常。PTLD 的異質性允許多樣化表現,從侷限性淋巴腺腫大至器官受累的散發性疾病456。
選項 (C):Monomorphic PTLD 比 polymorphic PTLD 預後差
Monomorphic PTLD 預後較 polymorphic 亞型差。NEJM 文獻透過治療算法證示此點:Polymorphic PTLD 常對減少免疫抑制(RIS)單獨治療有反應,應答率高,而 monomorphic PTLD—特別是非 DLBCL 亞型—需要更積極的治療,且「不適合作為唯一前期治療」單獨使用 RIS1。NCCN 指南同樣按組織學分層治療強度,monomorphic B 細胞 PTLD 需要 rituximab 及/或化學免疫治療前期治療,而非單獨 RIS3[^8]。一線治療失敗的高風險患者預後「仍然極差」56。
選項 (D):EBV-PTLD 可發生於非血液科的疾病及腫瘤設定
PTLD 發生於 固體器官移植(SOT)及造血幹細胞移植(HSCT),以及其他免疫抑制狀態。文獻一致將 PTLD 描述為「固體器官移植及造血幹細胞移植」的併發症456。美國移植學會指南特別論述「固體器官移植」2,SOT-PTLD 和 HSCT-PTLD 間的治療方式不同,RIS 在 SOT 中更有效於 HSCT1[^9]。
選項 (E):低強度化療合併 anti-CD20 單株抗體是標準治療
使用 rituximab (anti-CD20) 伴或不伴化療的風險分層序列方法代表 monomorphic 和 polymorphic B 細胞 PTLD 的標準治療範例456[^9]。NCCN 指南建議序列化學免疫治療,以 rituximab 開始,若 PET 陽性則進行 CHOP-R,或對虛弱患者同步化學免疫治療(CHOP-R 或減量方案 CEOP-R、CVP-R、GCVP-R)[^10]。此方法允許約 25% 的患者完全避免化療56。下列 NCCN 治療算法顯示此逐步策略:
從免疫抑制減少至 rituximab 再至化療的治療光譜進一步在此顯示:
NCCN 按 PTLD 亞型的一線治療算法:
參考文獻 (AMA)¶
-
Dierickx D, Habermann TM. Post-Transplantation Lymphoproliferative Disorders in Adults. The New England Journal of Medicine. 2018;378(6):549-562. doi:10.1056/NEJMra1702693. PMID:29414277. ↩↩↩↩↩↩↩↩↩↩
-
Allen UD, Preiksaitis JK, AST Infectious Diseases Community of Practice. Post-Transplant Lymphoproliferative Disorders, Epstein-Barr Virus Infection, and Disease in Solid Organ Transplantation: Guidelines From the American Society of Transplantation Infectious Diseases Community of Practice. Clinical Transplantation. 2019;33(9):e13652. doi:10.1111/ctr.13652. PMID:31230381. ↩↩↩↩↩↩↩↩
-
Atallah-Yunes SA, Salman O, Robertson MJ. Post-Transplant Lymphoproliferative Disorder: Update on Treatment and Novel Therapies. British Journal of Haematology. 2023;201(3):383-395. doi:10.1111/bjh.18763. PMID:36946218. ↩↩
-
Amengual JE, Pro B. How I Treat Posttransplant Lymphoproliferative Disorder. Blood. 2023;142(17):1426-1437. doi:10.1182/blood.2023020075. PMID:37540819. ↩↩↩↩↩↩
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=108. ↩↩↩↩↩↩↩↩↩↩
-
Michael J. Absalon,, Clifford Chin, Seth J. Rotz,, et al.. Post‐Transplant Malignancy and Lymphoproliferative Diseases. Transplantation and Mechanical Support for End‐Stage Heart and Lung Disease. 2023. Chapter 37 ISBN: 9781119633846. https://onlinelibrary.wiley.com/doi/10.1002/9781119633884.ch37. ↩↩↩↩↩↩↩↩↩↩
Figures¶