Q1. What is wrong description for large granular lymphocytic leukemia (LGLL)?¶
- (A) Typically, a chronic, indolent, lymphoproliferative disorder.
- (B) Most patients die of other comorbid conditions.
- (C) The main goal of therapy for most patients is cytoreduction of leukemic LGLs in the blood and marrow.
- (D) Associated autoimmune conditions requiring therapy is one of indications for LGLL therapy.
- (E) All of above are right.
點此顯示正解
(E) All of above are right.
詳解¶
Why (E) is the WRONG Answer¶
The question asks "What is wrong description for large granular lymphocytic leukemia?" — meaning the correct answer is the false statement. Option (E) "All of above are right" is the wrong answer because option (C) is false.
Why (C) is False:
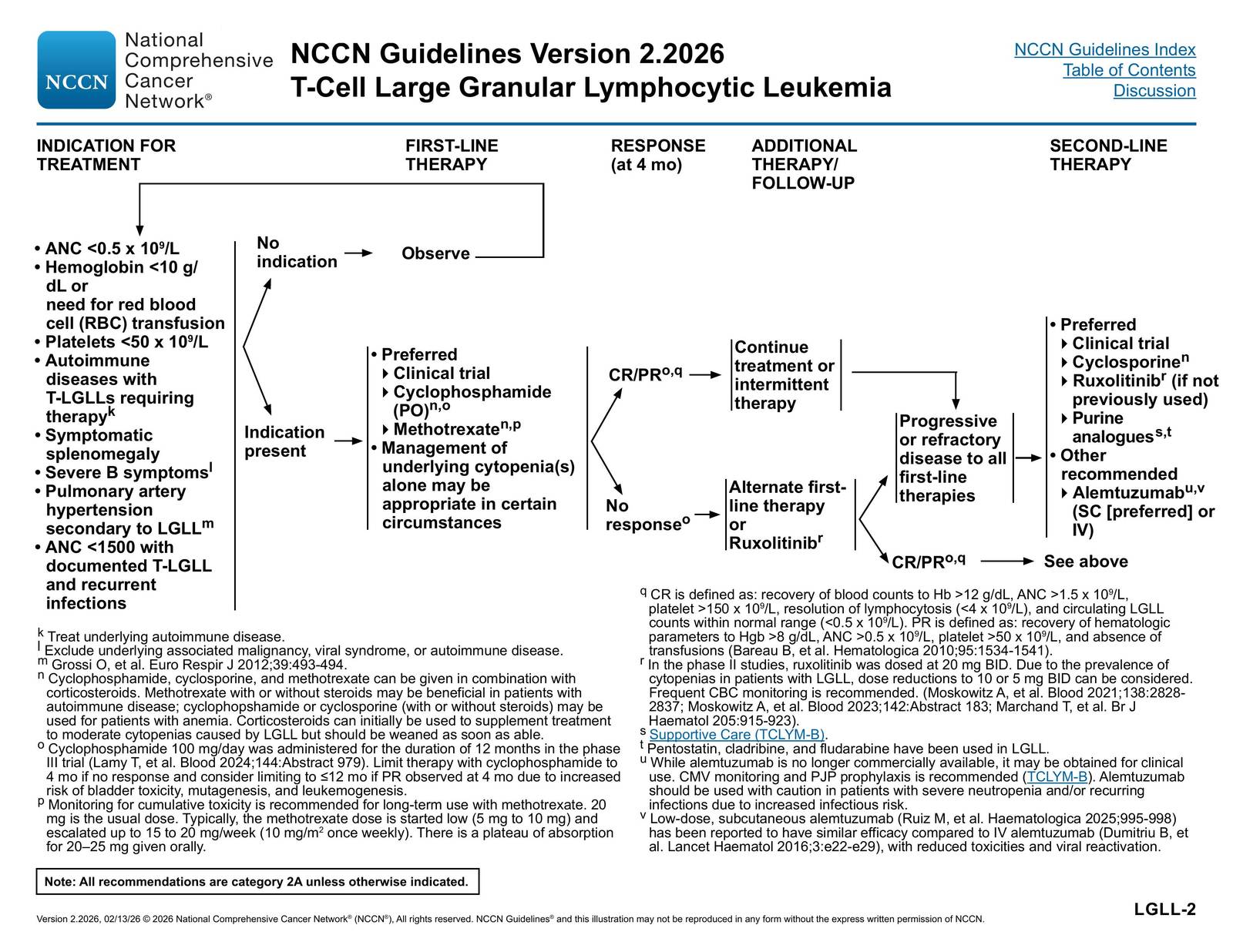
Option (C) states "The main goal of therapy for most patients is cytoreduction of leukemic LGLs in the blood and marrow." This is incorrect. The primary goal of LGLL therapy is not to reduce the leukemic clone burden, but rather to correct cytopenias and manage autoimmune complications1256.
The NCCN guidelines define treatment response based on hematologic recovery (hemoglobin >12 g/dL, ANC >1.5 × 10⁹/L, platelets >150 × 10⁹/L for complete response), not on reduction of LGL counts1. In fact, response criteria explicitly note that partial response requires only improvement in blood counts (Hgb >8 g/dL, ANC >0.5 × 10⁹/L) without requiring reduction in circulating LGL counts1[^8]. Multiple studies confirm that the degree of blood and bone marrow involvement does not correlate with disease severity or grade of cytopenias[^17], and treatment success is measured by clinical improvement in cytopenias and symptoms, not by clone reduction256.
The immunosuppressive agents used (methotrexate, cyclophosphamide, cyclosporine) target the immune dysregulation and cytopenia mechanisms rather than directly reducing the malignant clone2456. As one review states, LGLL treatment is "based on immunosuppressive therapy" because the pathogenic features involve chronic antigen-driven immune response and dysregulated apoptosis5.
Why the Other Options Are TRUE¶
Option (A): "Typically, a chronic, indolent, lymphoproliferative disorder" — TRUE
LGLL is consistently described as an indolent disease with a chronic course2[13][14][16][17]. The NCCN guidelines characterize it as "an indolent T-cell lymphoproliferative disorder" with "most cases hav[ing] an indolent and non-progressive clinical course"[^17]. The median survival is measured in years, and the disease follows a chronic pattern[7][16].
Option (B): "Most patients die of other comorbid conditions" — TRUE
LGLL has an indolent course with prolonged survival, and deaths are infrequently related to the disease itself5[^14]. One study of 319 patients showed median survival of 15.4 years overall, with female patients having even longer survival (median not reached)[^18]. The disease is characterized by long-term survival, and the literature emphasizes that "deaths infrequently occur because of infections related to severe neutropenia"5, implying most deaths are from other causes. The indolent nature and prolonged survival support that patients typically die of comorbid conditions rather than LGLL itself.
Option (D): "Associated autoimmune conditions requiring therapy is one of indications for LGLL therapy" — TRUE
Autoimmune diseases requiring therapy are explicitly listed as treatment indications in the NCCN guidelines1. The guidelines specify "Autoimmune diseases with T-LGLLs requiring therapy" as an indication for treatment1. Multiple studies confirm that autoimmune disorders (rheumatoid arthritis, Sjögren's syndrome, autoimmune cytopenias) are common in LGLL and represent treatment indications26[7][13][^16]. Methotrexate is specifically favored for patients with rheumatoid arthritis[^8], and treatment of underlying autoimmune disease is part of LGLL management1.
詳解 · 中文翻譯¶
為什麼 (E) 是錯誤的答案¶
題目要求「大顆粒淋巴細胞白血病 (LGLL) 的錯誤描述是什麼?」— 意味著正確答案是虛假的敘述。選項 (E)「上述都是對的」 是錯誤的答案,因為選項 (C) 是虛假的。
為什麼 (C) 是虛假的:
選項 (C) 陳述「大多數患者的治療主要目標是減少血液和骨髓中白血病 LGL 的細胞還原。」這是不正確的。LGLL 治療的主要目標不是減少白血病克隆負荷,而是糾正細胞減少症和管理自身免疫並發症1256。
NCCN 指南基於血液學恢復(血紅蛋白 >12 g/dL、ANC >1.5 × 10⁹/L、血小板 >150 × 10⁹/L 作為完全反應)定義治療反應,而不是 LGL 計數減少1。實際上,反應標準明確指出部分反應僅需改善血細胞計數(Hgb >8 g/dL、ANC >0.5 × 10⁹/L),不需要減少循環 LGL 計數1[8]。多項研究確認血液和骨髓累及程度與疾病嚴重性或細胞減少症程度不相關[17],治療成功由細胞減少症和症狀的臨床改善測量,而不是克隆還原256。
所使用的免疫抑制劑(甲氨蝶呤、環磷酰胺、環孢素)靶向免疫失調和細胞減少症機制,而不是直接減少惡性克隆2456。如一項綜述所述,LGLL 治療「基於免疫抑制治療」,因為病原特徵涉及慢性抗原驅動免疫反應和失調凋亡5。
為什麼其他選項是真實的¶
選項 (A):「通常,慢性、惰性的淋巴增殖性疾病」 — 真實
LGLL 一致地被描述為惰性疾病,具有慢性過程2[13][14][16][17]。NCCN 指南將其描述為「惰性 T 細胞淋巴增殖性疾病」,「大多數病例具有惰性和非進展臨床過程」[17]。中位存活期以年計,疾病遵循慢性模式[7][^16]。
選項 (B):「大多數患者死於其他併發症」 — 真實
LGLL 有惰性過程,存活期長,死亡很少與疾病本身相關5[^14]。對 319 名患者的一項研究顯示整體中位生存期為 15.4 年,女性患者甚至更長的存活期(中位未達到)[^18]。疾病的特徵是長期存活,文獻強調「死亡很少因中性粒細胞減少症引起的感染發生」5,暗示大多數死亡來自其他原因。惰性特性和延長存活支持患者通常死於併發症而不是 LGLL 本身。
選項 (D):「需要治療的相關自身免疫條件是 LGLL 治療的適應症之一」 — 真實
需要治療的自身免疫疾病在 NCCN 指南中明確列為治療適應症1。指南指定「需要治療的伴 T-LGLL 的自身免疫疾病」作為治療適應症1。多項研究確認自身免疫疾病(類風濕關節炎、Sjögren 症候群、自身免疫細胞減少症)在 LGLL 中常見,代表治療適應症26[7][13][16]。甲氨蝶呤特別青睞於類風濕關節炎患者[8],治療潛在自身免疫疾病是 LGLL 管理的一部分1。
參考文獻 (AMA)¶
-
National Comprehensive Cancer Network. T-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/t-cell.pdf#page=32. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Marchand T, Lamy T, Loughran TP. A Modern View of LGL Leukemia. Blood. 2024;144(18):1910-1923. doi:10.1182/blood.2023021790. PMID:38848524. ↩↩↩↩↩↩↩↩↩↩
-
Lamy T, Loughran TP. How I Treat LGL Leukemia. Blood. 2011;117(10):2764-74. doi:10.1182/blood-2010-07-296962. PMID:21190991. ↩
-
Marchand T, Pastoret C, Moignet A, Roussel M, Lamy T. Large Granular Lymphocyte Leukemia: A Clonal Disorder With Autoimmune Manifestations. Hematology. American Society of Hematology. Education Program. 2024;2024(1):143-149. doi:10.1182/hematology.2024000539. PMID:39644019. ↩↩
-
Dong N, Castillo Tokumori F, Isenalumhe L, et al. Large Granular Lymphocytic Leukemia - A Retrospective Study of 319 Cases. American Journal of Hematology. 2021;96(7):772-780. doi:10.1002/ajh.26183. PMID:33819354. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Zawit M, Bahaj W, Gurnari C, Maciejewski J. Large Granular Lymphocytic Leukemia: From Immunopathogenesis to Treatment of Refractory Disease. Cancers. 2021;13(17):4418. doi:10.3390/cancers13174418. PMID:34503230. ↩↩↩↩↩↩↩↩
Slide annotations
The most common indications for treatment are cytopenia, recurrent infection and pure red cell aplasia, progressive splenomegaly and B symptoms. There is currently no gold standard treatment for T-LGL leukemia. Most patients are treated with low doses of methotrexate, cyclophosphamide, and cyclosporine-A.
Figures¶