Q35. Which one of the followings is WRONG regarding NK/T-cell Lymphoma?¶
- (A) EBV infection is an essential diagnostic criterion.
- (B) Occurs primarily in the nose and upper airway (80%).
- (C) Quantification of plasma EBV is a prognostic factor.
- (D) Anthracycline regimens are effective for advanced disease.
- (E) EBV titer can be used for monitoring response to therapy.
點此顯示正解
(D) Anthracycline regimens are effective for advanced disease.
詳解¶
Board Exam Answer Analysis¶
Option (D) is FALSE because anthracycline-based regimens (such as CHOP) are ineffective for advanced extranodal NK/T-cell lymphoma due to high expression of MDR1/P-glycoprotein, which actively effluxes anthracyclines from tumor cells124. Complete remission rates with anthracycline-based chemotherapy are below 20%2. The standard of care for advanced disease consists of non-anthracycline asparaginase-containing regimens such as SMILE (dexamethasone, methotrexate, ifosfamide, L-asparaginase, etoposide), AspaMetDex, P-Gemox, and DDGP, which achieve response rates of 80% or higher25. NK/T-cell lymphomas express the multidrug resistance phenotype, rendering anthracycline-containing regimens ineffective4.
Why the other options are TRUE:
(A) EBV infection is an essential diagnostic criterion — TRUE. EBV infection in lymphoma cells is universal in NK/T-cell lymphoma48. The diagnosis is established with histological and immunohistochemical examination together with demonstration of EBV in tumor cells by in situ hybridization for EBV-encoded small RNA (EBER)48.
(B) Occurs primarily in the nose and upper airway (80%) — TRUE. Approximately 80% of extranodal NK/T-cell lymphoma patients present with upper aerodigestive tract involvement at initial diagnosis, including nasal cavity, nasopharynx, paranasal sinuses, and palate5. The most commonly involved site is the nasal cavity, followed by non-nasal sites including skin, gastrointestinal tract, and testis8.
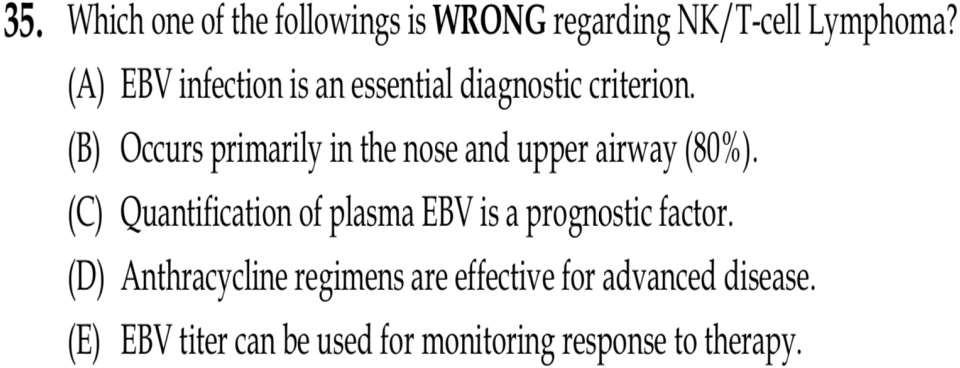
(C) Quantification of plasma EBV DNA is a prognostic factor — TRUE. Pretreatment plasma EBV DNA is an independent prognostic factor for overall survival and progression-free survival69. Detectable plasma EBV DNA at diagnosis is associated with higher clinical stage, presence of B symptoms, worse performance status, and significantly worse survival outcomes9. Multivariate analysis demonstrated that pretreatment plasma EBV DNA was a significant prognostic factor (hazard ratio 10.6)9.
(E) EBV titer can be used for monitoring response to therapy — TRUE. Plasma EBV DNA serves as a marker for treatment response and relapse monitoring7810. Plasma EBV DNA strongly correlates with lymphoma status and is more sensitive than PET/CT or CT/MRI for detecting relapse, with 97.1% sensitivity7. Achieving EBV DNA negativity during treatment is associated with better progression-free survival and overall survival10. Dynamic monitoring of plasma EBV DNA provides longitudinal prognostic information and therapeutic goals include achieving undetectable plasma EBV DNA410.
![Figure 1: The Association of EBV ‐ DNA Levels with Stages, Treatment Response, and Outcomes in Extranodal NK /T‐cell Lymphoma ( ENKTL ) Patients. A, Log [ EBV ‐ DNA ] Levels were Higher in Advanced Stage Patients Compared to Limited Stage Patients. B, Higher Log [ EBV ‐ DNA ] Levels were Observed in Patients without Response to Treatment Compared to Patients with Response to Treatment. C, Receiver Operating Characteristic Curve of Log [ EBV ‐ DNA ]. D, Progression‐Free Survival by Log [ EBV ‐ DNA ]. E, Overall Survival by Log [ EBV ‐ DNA ]](https://storage.googleapis.com/wiley-multimedia/cms/10.1111_ejh.13126/asset/b67ed31c-0aa4-497b-b82c-26eceed489ae/assets/images/large/ejh13126-fig-0001.jpg)
詳解 · 中文翻譯¶
棋盤考試答案分析¶
選項 (D) 假,因為 含蒽環類的方案(如 CHOP)對晚期結外 NK/T 細胞淋巴瘤無效,由於高表達 MDR1/P-糖蛋白,主動從腫瘤細胞中外流蒽環類124。含蒽環類化療的完全緩解率低於 20%2。晚期疾病的護理標準包括 非蒽環類含天冬酰胺酶方案,如 SMILE(地塞米松、甲氨蝶呤、異磷酰胺、L-天冬酰胺酶、依托泊苷)、AspaMetDex、P-Gemox 和 DDGP,達成 80% 或更高的反應率25。NK/T 細胞淋巴瘤表達多藥耐藥表型,使含蒽環類方案無效4。
其他選項為何真實:
(A) EBV 感染是必要診斷標準 — 真實。淋巴瘤細胞中的 EBV 感染在 NK/T 細胞淋巴瘤中通用48。診斷通過組織學和免疫組織化學檢查與通過原位雜交演示腫瘤細胞中的 EBV(EBV 編碼小 RNA [EBER])建立48。
(B) 主要發生在鼻子和上氣道(80%) — 真實。約 80% 的結外 NK/T 細胞淋巴瘤患者在初始診斷時呈現上消化道浸潤,包括鼻腔、鼻咽、副鼻竇和軟顎5。最常見浸潤位點是鼻腔,其次是包括皮膚、胃腸道和睾丸的非鼻位點8。
(C) 血漿 EBV DNA 量化是預後因素 — 真實。預治療血漿 EBV DNA 是整體生存和無進展生存的獨立預後因素69。診斷時可檢測血漿 EBV DNA 與更高臨床分期、B 症狀存在、更差表現狀態和顯著更差生存預後相關9。多變量分析證明預治療血漿 EBV DNA 是顯著預後因素(風險比 10.6)9。
(E) EBV 滴度可用於監測治療反應 — 真實。血漿 EBV DNA 作為治療反應和復發監測的標誌物7810。血漿 EBV DNA 強烈與淋巴瘤狀態相關,相比 PET/CT 或 CT/MRI 檢測復發更敏感,敏感性 97.1%7。在治療中達成 EBV DNA 陰性與更好的無進展生存和整體生存相關10。血漿 EBV DNA 的動態監測提供縱向預後信息,治療目標包括達成不可檢測血漿 EBV DNA410。
參考文獻 (AMA)¶
-
Yamaguchi M, Suzuki R, Oguchi M. Advances in the Treatment of Extranodal NK/T-cell Lymphoma, Nasal Type. Blood. 2018;131(23):2528-2540. doi:10.1182/blood-2017-12-791418. PMID:29602763. ↩↩
-
Shafiee A, Shamsi S, Kohandel Gargari O, et al. EBV Associated T- And NK-cell Lymphoproliferative Diseases: A Comprehensive Overview of Clinical Manifestations and Novel Therapeutic Insights. Reviews in Medical Virology. 2022;32(4):e2328. doi:10.1002/rmv.2328. PMID:35122349. ↩↩↩↩↩↩
-
Tse E, Zhao WL, Xiong J, Kwong YL. How We Treat NK/T-cell Lymphomas. Journal of Hematology & Oncology. 2022;15(1):74. doi:10.1186/s13045-022-01293-5. PMID:35659326. ↩
-
Wu W, Ren K, Chen X, et al. Comparison of the Clinical Efficacies of Two L-Asparaginase-Based Chemotherapy Regimens for Newly Diagnosed Nasal-Type Extranodal NK/T-cell Lymphoma. Cancer Medicine. 2023;12(8):9458-9470. doi:10.1002/cam4.5708. PMID:37000008. ↩↩↩↩↩↩↩↩↩↩
-
Tse E, Fox CP, Glover A, et al. Extranodal Natural Killer/T-Cell Lymphoma: An Overview on Pathology and Clinical Management. Seminars in Hematology. 2022;59(4):198-209. doi:10.1053/j.seminhematol.2022.10.002. PMID:36805888. ↩↩↩↩
-
Chan CY, Lin TL, Kuo MC, et al. Prognostic Impact of Pre-Treatment and Post-Treatment Plasma Epstein-Barr Virus DNA in Peripheral T-Cell Lymphomas. Annals of Medicine. 2025;57(1):2478315. doi:10.1080/07853890.2025.2478315. PMID:40110683. ↩↩
-
Suzuki R, Yamaguchi M, Izutsu K, et al. Prospective Measurement of Epstein-Barr Virus-Dna in Plasma and Peripheral Blood Mononuclear Cells of Extranodal NK/T-cell Lymphoma, Nasal Type. Blood. 2011;118(23):6018-22. doi:10.1182/blood-2011-05-354142. PMID:21984805. ↩↩↩↩
-
Yan Z, Yao Z, Wang H, et al. Plasma EBV-DNA and Peripheral Blood Mononuclear Cell EBV-DNA Have Disparate Clinical Relevance in Patients With Extranodal NK/T-cell Lymphoma. Journal of Clinical Virology : The Official Publication of the Pan American Society for Clinical Virology. 2022;157:105320. doi:10.1016/j.jcv.2022.105320. PMID:36240675. ↩↩↩↩↩↩↩↩
-
Chen Z, Huang H, Fang X, et al. Dynamic Monitoring of Circulating Cell-Free EBV-DNA for Risk Assessment in Early-Stage Natural Killer/T-Cell Lymphoma. Blood Advances. 2026;10(10):3457-3466. doi:10.1182/bloodadvances.2025018855. PMID:41824796. ↩↩↩↩↩↩
-
Su YJ, Wang PN, Chang H, et al. Extranodal NK/T-cell Lymphoma, Nasal Type: Clinical Features, Outcome, and Prognostic Factors in 101 Cases. European Journal of Haematology. 2018;101(3):379-388. doi:10.1111/ejh.13126. PMID:29908084. ↩↩↩↩↩↩
Figures¶