Q1. Which one of the followings is WRONG regarding Mantle Cell Lymphoma (MCL)?¶
- (A) MCL has a characteristic phenotype: CD5+, CD10- and CD23-.
- (B) MCL demonstrates t(11;14)(q13;q32) by karyotyping and FISH.
- (C) Expression of nuclear cyclin D1 protein in >90% of cases.
- (D) All MCL have an aggressive course.
- (E) Aggressive MCL has blastoid morphology and complex cytogenetics.
點此顯示正解
(D) All MCL have an aggressive course.
詳解¶
1. Why (D) is the WRONG statement¶
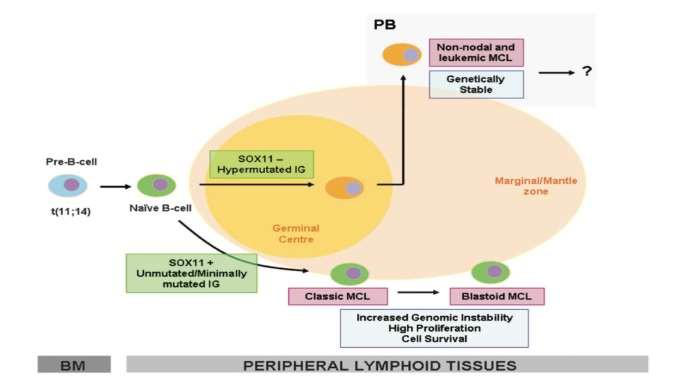
(D) is false because not all MCL has an aggressive course. MCL demonstrates significant clinical heterogeneity, with a well-characterized indolent leukemic non-nodal subtype that accounts for 10-20% of cases12. This indolent variant is characterized by:
- SOX11-negative immunophenotype134
- Mutated IGHV (immunoglobulin heavy chain variable region genes)135
- Leukemic non-nodal presentation (peripheral blood and bone marrow involvement without significant lymphadenopathy)14
- Low proliferation index (low Ki-67)24
- Lack of genomic complexity (fewer copy number alterations and structural variants)35
- Indolent clinical behavior with prolonged survival that may not require immediate treatment123
In the landmark study by Fernàndez et al., patients with SOX11-negative indolent MCL had a 5-year overall survival of 78% versus 36% for SOX11-positive conventional MCL (P = 0.001)3. These patients often exhibit nonnodal presentation, predominantly hypermutated IGHV, and noncomplex karyotypes, defining a specific subtype with excellent outcomes that can be managed conservatively with observation rather than immediate therapy3.
The WHO 2016 classification formally recognizes this dichotomy: conventional nodal MCL (80-90% of cases) with unmutated IGHV, SOX11 overexpression, and aggressive course versus leukemic non-nodal MCL (10-20% of cases) with mutated IGHV, SOX11 negativity, and indolent behavior15.
![Figure 1: FIG Understanding of the pathogenesis of mantle cell lymphoma (MCL) in 2022. Possible cell of origin for MCL is likely a B1a cell. Two major clinical presentations: common conventional MCL (90% of patients) with a generally aggressive clinical course and characterized by SOX‐11‐positive MCL cells and an unmutated immunoglobulin heavy chain variable region (IGHV), and an indolent clinical presentation of MCL (10% of patients), generally presenting as nonnodal leukemic‐phase MCL that is SOX‐11‐negative ( CCND1 and TLR2 mutations are frequent) and exhibits a germinal center reaction with somatic hypermutation of IGHV. Acquisition of other aberrant molecular changes such as TP53 , NSD2 , SMARCA4 , UBR5 , NOTCH2 , and CDKN2A deletions can further transform MCL into an aggressive blastoid or pleomorphic type of MCL (transformation in MCL). The presence of MCL clones in the inner mantle zone without disrupting the nodal architecture is considered in situ mantle cell neoplasia (ISMCN). Recently, DNA methylation patterns have further divided MCL into cluster 1 (common and aggressive) and cluster 2 (uncommon, indolent, and mutated IGHV). In the future, a combined clinico‐pathologic‐genomic approach will likely define subtypes of MCL. Major aberrations in the pathogenesis of MCL are summarized in the figure. Clinically, identifying the histology type; Ki‐67%; SOX‐11 status; karyotype; and somatic mutations in TP53 , ATM , CCND1 , NSD2 , NOTCH1 , NOTCH2 , SMARCA4 , and CDKN2A carry prognostic significance. (Adopted with permission from Reference 36 ) Abbreviations: IGHV (immunoglobulin heavy chain variable region) , SOX‐11 [sex‐determining region Y (SRY) (SRY‐related high mobility group‐box) protein] , PAX‐5 (paired box‐5) transcription factor , PDGF‐A (platelet derived growth factor‐A) , FAK kinase (focal adhesion kinase) , EpiCMIT score (epigenetically determined cumulative mitoses) , NSD2 (nuclear receptor binding SET domain protein 2) , KMT2D (lysine methyltransferase 2D) , SMARCA4/SWI complex (SWItch/sucrose nonfermentable) ATP dependent chromatin remodeling complex , OXPHOS (oxidative phosphorylation) pathway , BIRC3 (baculoviral IAP repeat containing 3) , TRAF2 (TNF receptor associated factor 2) , UBR5 (ubiquitin protein ligase E3 component N‐recognin 5) , HNRNPH (heterogeneous nuclear ribonucleoprotein H)](https://storage.googleapis.com/wiley-multimedia/cms/10.1002_ajh.26523/asset/994f2d76-b924-4549-a7ba-8fded82d564f/assets/images/large/ajh26523-fig-0001.jpg)
2. Why the other options are CORRECT¶
(A) MCL has a characteristic phenotype: CD5+, CD10-, CD23- — CORRECT
The classic immunophenotype of MCL is CD5+, CD10-, CD23- (also CD20+, Bcl-6-)8[9][10][^11]. This distinguishes MCL from chronic lymphocytic leukemia (CLL), which is typically CD5+, CD23+, and from follicular lymphoma, which is CD10+[^9]. However, it should be noted that SOX11-negative indolent MCL can be CD23+ in up to 39% of cases, though the classic phenotype remains CD23-negative4.
(B) MCL demonstrates t(11;14)(q13;q32) by karyotyping and FISH — CORRECT
The t(11;14)(q13;q32) translocation is the hallmark genetic abnormality of MCL, present in nearly all cases178[9][11]. This translocation juxtaposes the cyclin D1 gene (CCND1) at 11q13 with the immunoglobulin heavy chain gene enhancer at 14q32, resulting in constitutive cyclin D1 overexpression17[^9]. Detection of this translocation by FISH or karyotyping is crucial for diagnosis7[^11].
(C) Expression of nuclear cyclin D1 protein in >90% of cases — CORRECT
Cyclin D1 overexpression is detected by immunohistochemistry in >90% of MCL cases17. The t(11;14) translocation drives aberrant cyclin D1 expression, which is not normally expressed in lymphocytes8[^11]. Cyclin D1 is a cell-cycle regulatory protein that promotes G1-to-S phase transition7[^9]. Rare cyclin D1-negative cases exist and typically overexpress cyclin D2 or D3 instead8[9][11].
(E) Aggressive MCL has blastoid morphology and complex cytogenetics — CORRECT
Blastoid/pleomorphic morphology is associated with aggressive clinical behavior and high proliferation (high Ki-67)127. Blastoid variants are characterized by neoplastic cells resembling lymphoblasts and have a more aggressive clinical course17. Aggressive MCL is also characterized by complex cytogenetics and high genomic instability, including mutations in TP53, CDKN2A deletions, ATM mutations, and other aberrations that promote proliferation258[9][11]. These features contrast sharply with indolent MCL, which has stable genomes and fewer copy number alterations35.
詳解 · 中文翻譯¶
1. 為什麼 (D) 是錯誤的敘述¶
(D) 是假的因為並非所有 MCL 都有攻擊性病程。MCL 表現出顯著的臨床異質性,有一個眾所周知的惰性白血病性非結節性亞型佔10-20% 的病例12。此惰性變體的特徵是:
- SOX11 陰性免疫表型134
- 突變的 IGHV(免疫球蛋白重鏈可變區基因)135
- 白血病性非結節性表現(周邊血液和骨髓受累,無顯著淋巴結病變)14
- 低增殖指數(低 Ki-67)24
- 缺乏基因組複雜性(較少拷貝數改變和結構變異)35
- 惰性臨床行為具有可能不需要立即治療的延長生存123
在由 Fernàndez 等人進行的標誌性研究中,具有 SOX11 陰性惰性 MCL 的患者有 5 年總生存率為 78% vs 36% 用於 SOX11 陽性常規 MCL(P = 0.001)3。這些患者通常表現出非結節性表現,主要超突變 IGHV 和非複雜核型,定義一個具有優越結果的特定亞型,可通過觀察而不是立即療法保守地管理3。
WHO 2016 分類正式承認此二分法:常規結節性 MCL(80-90% 的病例)與未突變 IGHV、SOX11 過度表達和攻擊性病程 vs 白血病性非結節性 MCL(10-20% 的病例)與突變 IGHV、SOX11 陰性和惰性行為15。
2. 為什麼其他選項是正確的¶
(A) MCL 有特徵性表型:CD5+、CD10-、CD23- — 正確
MCL 的經典免疫表型是 CD5+、CD10-、CD23-(也是 CD20+、Bcl-6-)8[9][10][^11]。這區分 MCL 與慢性淋巴細胞白血病 (CLL),其通常為 CD5+、CD23+,和濾泡淋巴瘤,其為 CD10+[^9]。但應注意 SOX11 陰性惰性 MCL 可在最多 39% 的病例中為 CD23+,儘管經典表型保留為 CD23 陰性4。
(B) MCL 由核型和 FISH 證示 t(11;14)(q13;q32) — 正確
t(11;14)(q13;q32) 易位是 MCL 的標誌性遺傳異常,存在於幾乎所有病例中178[9][11]。此易位並置位於 11q13 的 cyclin D1 基因 (CCND1) 與位於 14q32 的免疫球蛋白重鏈基因增強子,導致本構型 cyclin D1 過度表達17[^9]。通過 FISH 或核型檢測此易位對於診斷至關重要7[^11]。
(C) >90% 的病例中核 cyclin D1 蛋白的表達 — 正確
Cyclin D1 過度表達由免疫組織化學在 >90% 的 MCL 病例中檢測17。t(11;14) 易位驅動異常 cyclin D1 表達,在淋巴細胞中通常不表達8[^11]。Cyclin D1 是一種細胞週期調控蛋白,促進 G1 至 S 期轉換7[^9]。罕見 cyclin D1 陰性病例存在,通常過度表達 cyclin D2 或 D3 代替8[9][11]。
(E) 攻擊性 MCL 有淋巴母細胞形態和複雜細胞遺傳學 — 正確
淋巴母細胞/多形態與攻擊性臨床行為和高增殖相關(高 Ki-67)127。淋巴母細胞變體的特徵是新生物細胞似淋巴母細胞且具有更攻擊性的臨床病程17。攻擊性 MCL 也由複雜細胞遺傳學和高基因組不穩定性特徵化,包括 TP53 中的突變、CDKN2A 缺失、ATM 突變和促進增殖的其他異常258[9][11]。這些特徵與惰性 MCL 形成鮮明對比,其具有穩定的基因組和較少的拷貝數改變35。
參考文獻 (AMA)¶
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Wilson MR, Barrett A, Cheah CY, Eyre TA. How I Manage Mantle Cell Lymphoma: Indolent Versus Aggressive Disease. British Journal of Haematology. 2023;201(2):185-198. doi:10.1111/bjh.18697. PMID:36807902. ↩↩↩↩↩↩↩↩↩↩
-
Fernàndez V, Salamero O, Espinet B, et al. Genomic and Gene Expression Profiling Defines Indolent Forms of Mantle Cell Lymphoma. Cancer Research. 2010;70(4):1408-18. doi:10.1158/0008-5472.CAN-09-3419. PMID:20124476. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Xu J, Wang L, Li J, et al. SOX11-negative Mantle Cell Lymphoma: Clinicopathologic and Prognostic Features of 75 Patients. The American Journal of Surgical Pathology. 2019;43(5):710-716. doi:10.1097/PAS.0000000000001233. PMID:30768440. ↩↩↩↩↩↩↩↩
-
Jain P, Wang ML. Mantle Cell Lymphoma in 2022-a Comprehensive Update on Molecular Pathogenesis, Risk Stratification, Clinical Approach, and Current and Novel Treatments. American Journal of Hematology. 2022;97(5):638-656. doi:10.1002/ajh.26523. PMID:35266562. ↩↩↩↩↩↩↩↩↩↩
-
Vose JM. Mantle Cell Lymphoma: 2017 Update on Diagnosis, Risk-Stratification, and Clinical Management. American Journal of Hematology. 2017;92(8):806-813. doi:10.1002/ajh.24797. PMID:28699667. ↩
-
Armitage JO, Longo DL. Mantle-Cell Lymphoma. The New England Journal of Medicine. 2022;386(26):2495-2506. doi:10.1056/NEJMra2202672. PMID:35767440. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Vose JM. Mantle Cell Lymphoma: 2015 Update on Diagnosis, Risk-Stratification, and Clinical Management. American Journal of Hematology. 2015;90(8):739-45. doi:10.1002/ajh.24094. PMID:26103436. ↩↩↩↩↩↩↩↩↩↩
Figures¶