Q1. Which one of the following descriptions for hypercalcemia of malignancy is wrong?¶
- (A) It could be due to osteolytic bone lesions.
- (B) Patients typically become symptomatic when serum calcium exceeds 12 mg/dL (3 mmol/L).
- (C) Renal calcium excretion should be increased by aggressive IV hydration with normal saline and use of furosemide.
- (D) Calcium mobilization from bone should be decreased by bisphosphonates.
- (E) Immobilization per se does not aggravate hypercalcemia.
點此顯示正解
(E) Immobilization per se does not aggravate hypercalcemia.
詳解¶
Why Statement (E) is WRONG¶
Statement (E) claims that "immobilization per se does not aggravate hypercalcemia" — this is incorrect. Immobilization does aggravate hypercalcemia in malignancy. When patients are immobilized, reduced weight-bearing and muscle activity decrease mechanical stress on bone, which reduces osteoblast-mediated bone formation. However, bone resorption by osteoclasts continues unopposed, releasing additional calcium into the circulation and worsening hypercalcemia. This is why mobilization (when clinically feasible) is considered part of supportive management for hypercalcemia of malignancy, while prolonged bedrest exacerbates the condition. The statement is therefore false, making it the correct answer to this "which is WRONG" question.
Why Statements (A), (B), (C), and (D) are CORRECT¶
(A) Osteolytic bone lesions cause hypercalcemia — Correct. Local osteolytic hypercalcemia results from direct tumor invasion of bone with release of cytokines and growth factors that stimulate osteoclast-mediated bone resorption. This mechanism is seen in multiple myeloma, breast cancer with bone metastases, and other solid tumors with skeletal involvement13[^6].
(B) Symptoms typically begin when calcium exceeds 12 mg/dL (3 mmol/L) — Correct. Most patients remain asymptomatic with mild hypercalcemia but develop symptoms when corrected calcium rises above 12 mg/dL. Severe symptoms (altered mental status, confusion) typically occur when calcium exceeds 13-14 mg/dL, prompting urgent treatment3[^5].
(C) Aggressive IV saline hydration and furosemide increase renal calcium excretion — Correct (though the role of furosemide is now controversial). Isotonic saline hydration (200-500 mL/hour) is first-line therapy, correcting volume depletion and enhancing urinary calcium excretion by increasing glomerular filtration rate123[^7]. Loop diuretics like furosemide increase calciuresis by inhibiting calcium reabsorption in the thick ascending loop of Henle. However, current guidelines emphasize that furosemide should only be used after volume repletion and primarily in patients at risk for volume overload, as premature use can worsen dehydration and hypercalcemia123[^7]. The Endocrine Society notes "very little evidence to support the efficacy and safety" of furosemide in hypercalcemia of malignancy[^6]. Despite this evolving view, the statement remains technically correct that furosemide increases renal calcium excretion when used appropriately.
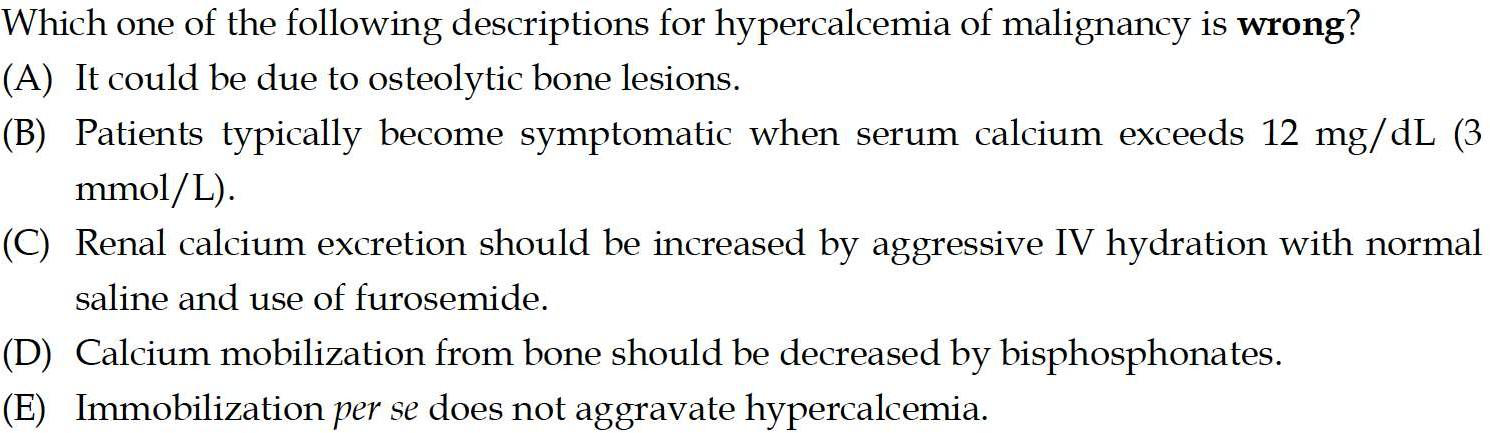
(D) Bisphosphonates decrease calcium mobilization from bone — Correct. Intravenous bisphosphonates (pamidronate 60-90 mg, zoledronic acid 4 mg) are potent inhibitors of osteoclast-mediated bone resorption and represent first-line antiresorptive therapy for hypercalcemia of malignancy123[^7]. Pamidronate and zoledronic acid inhibit farnesyl pyrophosphate synthase within osteoclasts, causing osteoclast apoptosis and reducing bone resorption. Zoledronic acid normalizes calcium in 80-90% of patients over 48-72 hours with a median duration of 30-40 days; pamidronate normalizes calcium in 60-70% with median duration of 11-14 days3[^9]. Denosumab (120 mg subcutaneously) is an alternative RANKL inhibitor that also reduces bone resorption13[^4].
詳解 · 中文翻譯¶
為什麼敘述 (E) 是錯誤的¶
敘述 (E) 聲稱「固定本身不會加重高鈣血症」— 這是不正確的。固定確實在惡性腫瘤中加重高鈣血症。當患者固定時,減少的負重和肌肉活動降低骨上的機械應力,減少成骨細胞介導的骨形成。但是,破骨細胞的骨吸收繼續無反對進行,向循環釋放額外的鈣並惡化高鈣血症。這就是為什麼活動(在臨床上可行時)被認為是惡性腫瘤高鈣血症支持治療的一部分,而長期臥床使病況惡化。因此陳述是假的,使其成為此「哪個是錯誤的」問題的正確答案。
為什麼敘述 (A)、(B)、(C) 和 (D) 是正確的¶
(A) 骨溶解性骨病變造成高鈣血症 — 正確。局部骨溶解性高鈣血症由腫瘤直接侵犯骨導致,釋放細胞因子和生長因子刺激破骨細胞介導的骨吸收。這種機制見於多發性骨髓瘤、有骨轉移的乳腺癌和其他伴有骨骼受累的實體腫瘤13[^6]。
(B) 血鈣超過 12 mg/dL(3 mmol/L)時症狀通常開始出現 — 正確。大多數患者在輕度高鈣血症時仍無症狀,但當校正血鈣升高超過 12 mg/dL 時出現症狀。嚴重症狀(精神狀態改變、混亂)通常在血鈣超過 13-14 mg/dL 時出現,促使急迫治療3[^5]。
(C) 積極靜脈鹽水水合和呋塞米增加腎臟鈣排泄 — 正確(儘管呋塞米的作用現在是有爭議的)。等滲鹽水水合(200-500 mL/小時)是一線療法,糾正體積耗盡並通過增加腎小球濾過率增強尿鈣排泄123[^7]。迴圈利尿藥如呋塞米通過在 Henle 粗上升管中抑制鈣重吸收增加降鈣尿。但是,當前指南強調呋塞米應僅在體積補充後使用,主要用於處於體積超負荷風險的患者,因為過早使用可能惡化脫水和高鈣血症123[7]。內分泌學會注意到「非常少的證據支持呋塞米的療效和安全性」在惡性腫瘤高鈣血症中[6]。儘管這種演變中的觀點,當適當使用時,陳述仍然在技術上正確呋塞米增加腎臟鈣排泄。
(D) 二磷酸鹽減少骨鈣動員 — 正確。靜脈注射二磷酸鹽(帕米膦酸 60-90 mg、唑來膦酸 4 mg)是破骨細胞介導的骨吸收的有力抑制劑,代表惡性腫瘤高鈣血症的一線抗吸收療法123[^7]。帕米膦酸和唑來膦酸在破骨細胞內抑制遠端焦磷酸合酶,引起破骨細胞凋亡並減少骨吸收。唑來膦酸在 48-72 小時內在 80-90% 患者中使血鈣正常化,中位持續時間為 30-40 天;帕米膦酸在 60-70% 中使血鈣正常化,中位持續時間為 11-14 天3[^9]。地舒單抗(120 mg 皮下注射)是替代 RANKL 抑制劑,也減少骨吸收13[^4]。
參考文獻 (AMA)¶
-
El-Hajj Fuleihan G, Clines GA, Hu MI, et al. Treatment of Hypercalcemia of Malignancy in Adults: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology and Metabolism. 2023;108(3):507-528. doi:10.1210/clinem/dgac621. PMID:36545746. ↩↩↩↩↩↩↩↩↩↩
-
Guise TA, Wysolmerski JJ. Cancer-Associated Hypercalcemia. The New England Journal of Medicine. 2022;386(15):1443-1451. doi:10.1056/NEJMcp2113128. PMID:35417639. ↩↩↩↩↩↩
-
Walker MD, Shane E. Hypercalcemia: A Review. Jama. 2022;328(16):1624-1636. doi:10.1001/jama.2022.18331. PMID:36282253. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩
Figures¶