Q25. Which of the following diseases is the most common secondary primary malignancy after CAR-T therapy?¶
- (A) MDS and AML
- (B) T cell lymphoma
- (C) B cell lymphoma
- (D) Skin cancers
- (E) Lung cancers
點此顯示正解
(A) MDS and AML
詳解¶
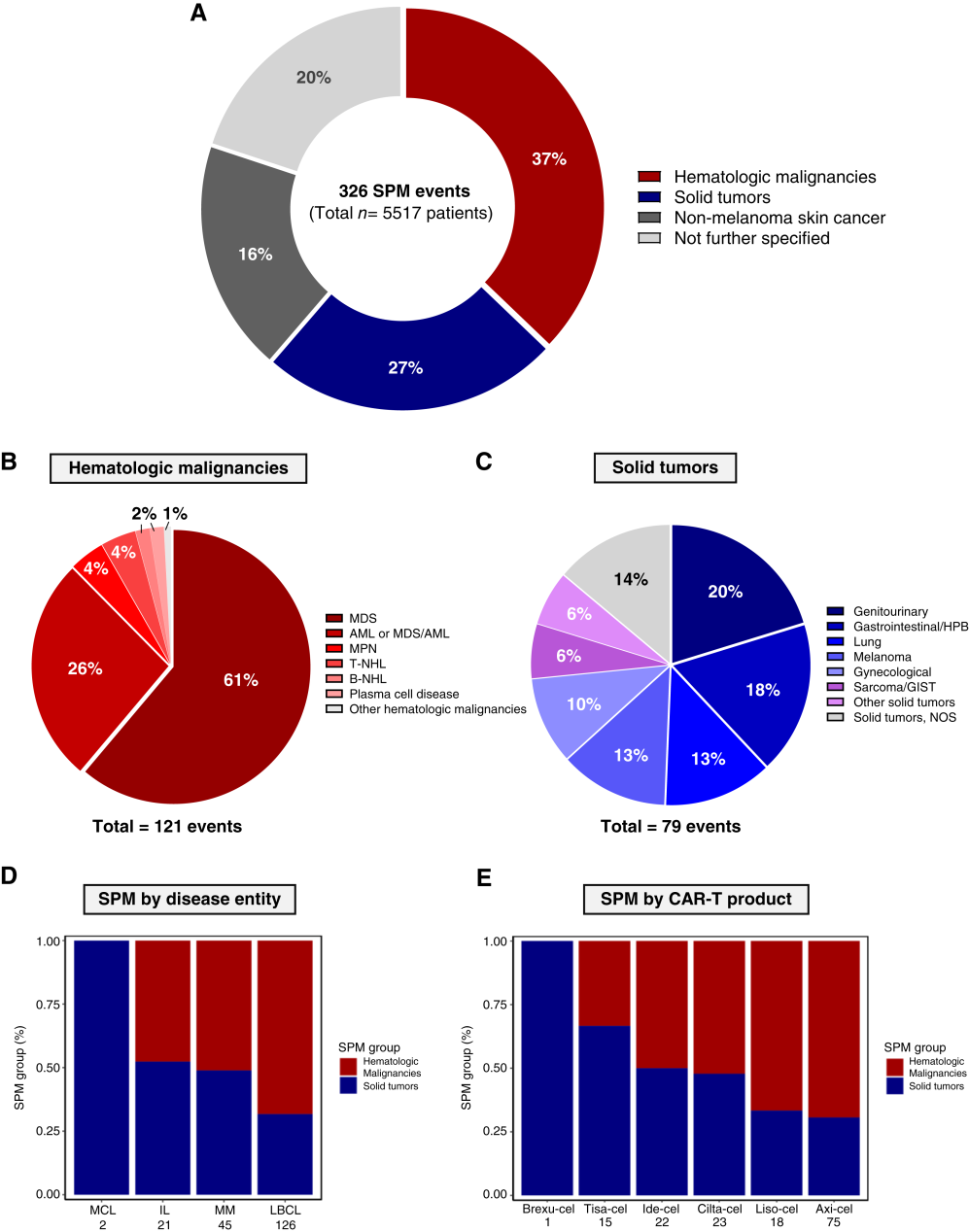
Therapy-related myeloid neoplasms (t-MDS/t-AML) are the most common second primary malignancies after CAR-T cell therapy, accounting for the largest proportion of hematologic SPMs, which collectively represent 37% of all SPMs.1 The correct answer is (A) MDS and AML.
Why (A) MDS and AML is Correct¶
The 2024 systematic review and meta-analysis in Clinical Cancer Research by Tix et al. analyzed 326 SPMs across 5,517 lymphoma and myeloma patients receiving CAR-T therapy.1 Hematologic malignancies were the most common SPM category (37% of all SPMs), with myeloid neoplasms predominating within this group.1 Specifically, myelodysplastic syndrome (MDS) incidence ranges from 0.3% to 4.2%, and acute myeloid leukemia (AML) from 0.2% to 1.1% of CAR-T recipients.2 Overall, secondary myeloid malignancies affect approximately 2% to 10% of patients within 5 years after CAR-T infusion.3
The mechanism is primarily attributed to prior cytotoxic chemotherapy exposure rather than CAR-T therapy itself. Patients receiving CAR-T have typically undergone multiple lines of prior therapy, including alkylating agents and purine analogs (such as fludarabine used in lymphodepletion), which are known mutagens.3[^7] Studies demonstrate that clonal hematopoiesis (CH) is often detectable before CAR-T infusion, with pre-existing myeloid clones expanding post-therapy.[^7] Among 40 evaluable patients, 46 CH clones were detected pre–CAR-T and 51 post–CAR-T, suggesting CAR-T may promote expansion of existing clones rather than creating new ones.[^7] Importantly, randomized trials comparing CAR-T to standard-of-care showed similar SPM risk (P = 0.92), indicating the myeloid neoplasm risk is not uniquely attributable to CAR-T itself.1
Why the Other Options Are Incorrect¶
(B) T-cell lymphoma: While T-cell lymphomas generated significant regulatory attention following an FDA boxed warning in November 2023, they remain exceedingly rare. The FDA identified only 20 cases among approximately 30,000 CAR-T recipients (0.067%).[5][7] In the Tix meta-analysis, T-cell malignancies represented only 1.5% of all SPMs.1 Across commercially approved CAR-T products, T-cell cancer incidence ranges from 0.03% to 1%.2[^10] Despite the FDA safety communication, the absolute numbers are far lower than myeloid neoplasms.
(C) B-cell lymphoma: B-cell lymphomas are not prominently reported as SPMs after CAR-T therapy. The literature focuses on myeloid neoplasms, solid tumors, and non-melanoma skin cancers as the predominant SPM categories.1 B-cell lymphomas would be difficult to distinguish from relapsed primary disease in patients treated for B-cell malignancies.
(D) Skin cancers: Non-melanoma skin cancers account for 16% of all SPMs in the meta-analysis,1 making them the third most common category after hematologic malignancies (37%) and solid tumors (27%). While clinically relevant, they are less frequent than myeloid neoplasms.
(E) Lung cancers: Solid tumors collectively represent 27% of SPMs,1 but no single solid tumor type (including lung cancer) predominates. The distribution of solid tumors is heterogeneous and does not appear limited to a particular diagnosis.2 Myeloid neoplasms remain more common than any individual solid tumor type.
The following figure illustrates the spectrum of SPMs across all FDA-approved CAR-T products, showing myeloid cancers as a major transgene-negative SPC category:

詳解 · 中文翻譯¶
治療相關骨髓新生物(t-MDS/t-AML)是 CAR-T 細胞治療後最常見的第二原發惡性腫瘤,佔血液腫瘤 SPM 的最大比例,其整體代表所有 SPM 的 37%。1 正確答案是 (A) MDS 和 AML。
為什麼 (A) MDS 和 AML 正確¶
2024 年在《臨床癌症研究》中由 Tix 等人進行的系統綜述和統合分析分析了 5,517 名接受 CAR-T 治療的淋巴瘤和骨髓瘤患者中的 326 個 SPM。1 血液惡性腫瘤是最常見的 SPM 類別(所有 SPM 的 37%),骨髓新生物在此類別中占主導。1 具體而言,骨髓發育不良綜合症(MDS)發生率從 0.3% 至 4.2%,急性髓性白血病(AML)從 0.2% 至 1.1% 的 CAR-T 接受者。2 整體而言,繼發性骨髓惡性腫瘤在 CAR-T 輸注後 5 年內影響約 2% 至 10% 的患者。3
該機制主要歸因於先前的細胞毒性化療暴露而不是 CAR-T 治療本身。接受 CAR-T 的患者通常已經接受多線先前治療,包括烷化劑和嘌呤類似物(如用於淋巴耗盡的氟達拉濱),這些是已知的誘變劑。3[^7] 研究證明克隆造血(CH)經常可在 CAR-T 輸注前檢測到,預先存在的骨髓克隆在治療後擴張。[^7] 在 40 名可評估患者中,檢測到 46 個 CH 克隆前-CAR-T 和 51 個後-CAR-T,表明 CAR-T 可能促進現有克隆的擴張而不是產生新的克隆。[^7] 重要地是,比較 CAR-T 與標準護理的隨機試驗顯示相似的 SPM 風險(P = 0.92),表明骨髓新生物風險不是唯一歸因於 CAR-T 本身。1
為什麼其他選項是不正確的¶
(B) T 細胞淋巴瘤:雖然 T 細胞淋巴瘤在 2023 年 11 月 FDA 方盒警告後引起了重大監管關注,它們仍然極其罕見。FDA 在約 30,000 名 CAR-T 接受者中僅識別了 20 例(0.067%)。[5][7] 在 Tix 統合分析中,T 細胞惡性腫瘤代表僅所有 SPM 的 1.5%。1 在商業批准的 CAR-T 產品中,T 細胞癌發生率從 0.03% 至 1%。2[^10] 儘管有 FDA 安全通訊,絕對數字遠低於骨髓新生物。
(C) B 細胞淋巴瘤:B 細胞淋巴瘤未被突出報告為 CAR-T 治療後的 SPM。文獻集中於骨髓新生物、實心腫瘤和非黑色素瘤皮膚癌作為主導的 SPM 類別。1 B 細胞淋巴瘤難以從用 B 細胞惡性腫瘤治療的患者中復發的原發疾病區分。
(D) 皮膚癌:非黑色素瘤皮膚癌在統合分析中佔所有 SPM 的 16%,1 使其成為在血液惡性腫瘤(37%)和實心腫瘤(27%)之後的第三最常見類別。雖然臨床相關,它們比骨髓新生物更不常見。
(E) 肺癌:實心腫瘤整體代表 SPM 的 27%,1 但沒有單一實心腫瘤類型(包括肺癌)占主導。實心腫瘤的分佈是異質的,似乎不限於特定診斷。2 骨髓新生物仍比任何單個實心腫瘤類型更常見。
參考文獻 (AMA)¶
-
Tix T, Alhomoud M, Shouval R, et al. Second Primary Malignancies After CAR T-Cell Therapy: A Systematic Review and Meta-Analysis of 5,517 Lymphoma and Myeloma Patients. Clinical Cancer Research : An Official Journal of the American Association for Cancer Research. 2024;30(20):4690-4700. doi:10.1158/1078-0432.CCR-24-1798. PMID:39256908. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Mohty R, Halwani A, Badar T, et al. Malignancies After Chimeric Antigen Receptor T Cell Therapy. Transplantation and Cellular Therapy. 2025;:S2666-6367(25)01218-7. doi:10.1016/j.jtct.2025.06.001. PMID:40482820. ↩↩↩↩↩↩
-
Brudno JN, Maus MV, Hinrichs CS. CAR T Cells and T-Cell Therapies for Cancer: A Translational Science Review. Jama. 2024;332(22):1924-1935. doi:10.1001/jama.2024.19462. PMID:39495525. ↩↩↩↩
-
Patel SA, Spiegel JY, Dahiya S. Second Primary Cancer After Chimeric Antigen Receptor-T-Cell Therapy: A Review. JAMA Oncology. 2025;11(2):174-181. doi:10.1001/jamaoncol.2024.5412. PMID:39666320. ↩
Slide annotations
Clin Cancer Res (2024) 30 (20): 4690–4700.
Figures¶