Q14. Which following statement about Mantle cell lymphoma (MCL) is WRONG?¶
- (A) Clinical indolent MCL often includes biomarkers of unmutated IGHV and lack of SOX11 and TP53.
- (B) Frontline cytarabine-based chemoimmunotherapy regimen followed by autologous HCT and maintenance with an anti-CD20 antibody is the standard of care approach in younger and fit patients.
- (C) TRIANGLE trial demonstrated efficacy of first line fixed duration of ibrutinib among young and fit patients.
- (D) BOVEN trial demonstrated efficacy of zanubrutinib, obinutuzumab and venetoclax as first line treatment in TP53 mutated MCL.
- (E) All above are correct.
點此顯示正解
(A) Clinical indolent MCL often includes biomarkers of unmutated IGHV and lack of SOX11 and TP53.
詳解¶
Answer¶
Option (A) is the WRONG statement because clinically indolent MCL is characterized by mutated IGHV (not unmutated), SOX11 negativity, and typically TP53 wild-type status. The statement incorrectly lists "unmutated IGHV" as a feature of indolent MCL, when this is actually a hallmark of conventional aggressive MCL.
1. Why (A) is incorrect — the molecular profile of indolent MCL¶
Indolent (leukemic non-nodal) MCL represents 10-20% of cases and displays a distinct molecular signature123:
- Mutated IGHV (often hypermutated with <95% germline identity): Indolent MCL arises from germinal center-experienced B cells with somatic hypermutation, contrasting with conventional MCL which has unmutated IGHV genes123
- SOX11 negativity: Absence of SOX11 expression is a defining feature of indolent MCL and correlates with better outcomes (5-year OS 78% vs 36% for SOX11-positive)3
- TP53 wild-type: Indolent MCL typically lacks TP53 mutations and has less genomic complexity overall35
- Non-nodal presentation: Usually presents with leukemic disease rather than nodal involvement12
In contrast, conventional aggressive MCL (80-90% of cases) is characterized by unmutated IGHV, SOX11 positivity, nodal presentation, and more aggressive clinical behavior14. The statement in option (A) incorrectly attributes the molecular features of aggressive MCL to the indolent subtype.
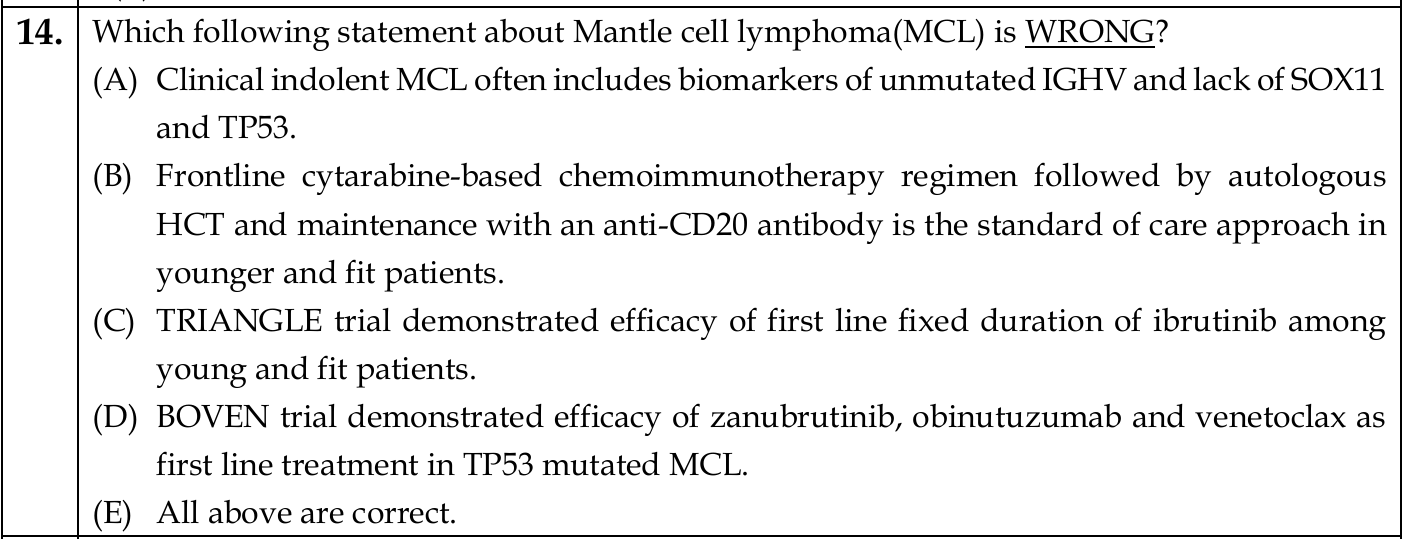
![Figure 1: FIG Understanding of the pathogenesis of mantle cell lymphoma (MCL) in 2022. Possible cell of origin for MCL is likely a B1a cell. Two major clinical presentations: common conventional MCL (90% of patients) with a generally aggressive clinical course and characterized by SOX‐11‐positive MCL cells and an unmutated immunoglobulin heavy chain variable region (IGHV), and an indolent clinical presentation of MCL (10% of patients), generally presenting as nonnodal leukemic‐phase MCL that is SOX‐11‐negative ( CCND1 and TLR2 mutations are frequent) and exhibits a germinal center reaction with somatic hypermutation of IGHV. Acquisition of other aberrant molecular changes such as TP53 , NSD2 , SMARCA4 , UBR5 , NOTCH2 , and CDKN2A deletions can further transform MCL into an aggressive blastoid or pleomorphic type of MCL (transformation in MCL). The presence of MCL clones in the inner mantle zone without disrupting the nodal architecture is considered in situ mantle cell neoplasia (ISMCN). Recently, DNA methylation patterns have further divided MCL into cluster 1 (common and aggressive) and cluster 2 (uncommon, indolent, and mutated IGHV). In the future, a combined clinico‐pathologic‐genomic approach will likely define subtypes of MCL. Major aberrations in the pathogenesis of MCL are summarized in the figure. Clinically, identifying the histology type; Ki‐67%; SOX‐11 status; karyotype; and somatic mutations in TP53 , ATM , CCND1 , NSD2 , NOTCH1 , NOTCH2 , SMARCA4 , and CDKN2A carry prognostic significance. (Adopted with permission from Reference 36 ) Abbreviations: IGHV (immunoglobulin heavy chain variable region) , SOX‐11 [sex‐determining region Y (SRY) (SRY‐related high mobility group‐box) protein] , PAX‐5 (paired box‐5) transcription factor , PDGF‐A (platelet derived growth factor‐A) , FAK kinase (focal adhesion kinase) , EpiCMIT score (epigenetically determined cumulative mitoses) , NSD2 (nuclear receptor binding SET domain protein 2) , KMT2D (lysine methyltransferase 2D) , SMARCA4/SWI complex (SWItch/sucrose nonfermentable) ATP dependent chromatin remodeling complex , OXPHOS (oxidative phosphorylation) pathway , BIRC3 (baculoviral IAP repeat containing 3) , TRAF2 (TNF receptor associated factor 2) , UBR5 (ubiquitin protein ligase E3 component N‐recognin 5) , HNRNPH (heterogeneous nuclear ribonucleoprotein H)](https://storage.googleapis.com/wiley-multimedia/cms/10.1002_ajh.26523/asset/994f2d76-b924-4549-a7ba-8fded82d564f/assets/images/large/ajh26523-fig-0001.jpg)
2. Why the other options are correct¶
(B) Frontline cytarabine-based chemoimmunotherapy + ASCT + anti-CD20 maintenance is standard of care in young/fit patients
This has been the established standard approach for transplant-eligible patients ≤65 years79. Cytarabine-containing regimens (such as R-CHOP alternating with R-DHAP) followed by ASCT and rituximab maintenance have demonstrated improved long-term outcomes compared to standard immunochemotherapy alone9. This remains a valid standard of care approach, though the TRIANGLE trial has now shown that adding ibrutinib to this regimen improves outcomes further78.
(C) TRIANGLE trial demonstrated efficacy of first-line fixed-duration ibrutinib in young/fit patients
The TRIANGLE trial (European MCL Network, published 2024 with 4.5-year follow-up in 2026) demonstrated that adding fixed-duration ibrutinib (during induction and as 2-year maintenance) to R-CHOP/R-DHAP significantly improved both failure-free survival and overall survival in transplant-eligible patients aged 18-65 years789. Notably, the trial showed that ibrutinib-containing immunochemotherapy without ASCT achieved non-inferior outcomes compared to the ASCT arm, with the ibrutinib-without-ASCT arm showing superior efficacy and less toxicity than standard ASCT alone8[^11]. This represents a paradigm shift in frontline MCL management.
(D) BOVEN trial demonstrated efficacy of zanubrutinib + obinutuzumab + venetoclax in TP53-mutated MCL
The BOVEN phase 2 trial (reported 2025) evaluated the triple combination of zanubrutinib (second-generation BTK inhibitor), venetoclax (BCL2 inhibitor), and obinutuzumab (anti-CD20 antibody) specifically in patients with TP53-mutated MCL[^10]. This high-risk population typically has poor outcomes with conventional chemotherapy. The trial demonstrated excellent results with 72% progression-free survival and 76% overall survival at 2 years, with good tolerability[^10]. This represents an important chemotherapy-free option for this particularly challenging patient subset.
詳解 · 中文翻譯¶
答案¶
選項 (A) 是錯誤的敘述,因為臨床上惰性的 MCL 的特徵是 TP53 突變的 IGHV(而不是未突變)、SOX11 陰性,以及通常 TP53 野生型狀態。敘述錯誤地列舉「未突變 IGHV」作為惰性 MCL 的特徵,而這實際上是傳統侵襲性 MCL 的特徵。
1. 為什麼 (A) 是不正確的 — 惰性 MCL 的分子型態¶
惰性(白血病非結節性)MCL 代表 10-20% 的病例,並呈現不同的分子簽名123:
- 突變型 IGHV(通常超突變,<95% 種系同源性):惰性 MCL 源自具有體細胞超突變的生發中心經驗 B 細胞,與傳統 MCL 相對比,後者具有未突變 IGHV 基因123
- SOX11 陰性:SOX11 表達的缺失是惰性 MCL 的定義特徵,與更好的預後相關(5 年 OS 78% vs SOX11 陽性的 36%)3
- TP53 野生型:惰性 MCL 通常缺乏 TP53 突變,整體基因組複雜性較少35
- 非結節性呈現:通常以白血病病呈現而不是結節累及12
相比之下,傳統侵襲性 MCL(80-90% 的病例)的特徵是 未突變 IGHV、SOX11 陽性、結節呈現和更侵襲性的臨床行為14。選項 (A) 中的敘述錯誤地將侵襲性 MCL 的分子特徵歸因於惰性亞型。
2. 為什麼其他選項是正確的¶
(B) 一線細胞阿糖苷基礎化療免疫治療 + ASCT + 抗-CD20 維持是年輕/健身患者的標準護理
這一直是移植合格患者 ≤65 歲的既定標準方法79。細胞阿糖苷含有方案(如交替的 R-CHOP 和 R-DHAP),隨後進行 ASCT 和利妥昔單抗維持,相比單獨標準免疫化療已證明改善長期結果9。這仍然是有效的標準護理方法,儘管 TRIANGLE 試驗現已顯示向此方案添加 ibrutinib 進一步改善結果78。
(C) TRIANGLE 試驗在年輕/健身患者中展示一線固定持續時間 ibrutinib 的療效
TRIANGLE 試驗(歐洲 MCL 網絡,2024 年發表,2026 年 4.5 年隨訪)證明向 R-CHOP/R-DHAP 添加 固定持續時間 ibrutinib(歸納期間和 2 年維持)在 18-65 歲移植符合條件患者中明顯改善無故障生存期和整體存活率789。值得注意的是,試驗顯示 ibrutinib 含免疫化療 不含 ASCT 相比 ASCT 臂實現了非劣效結果,不含 ASCT 的 ibrutinib 臂相比單獨標準 ASCT 顯示優越療效和更少毒性8[^11]。這代表一線 MCL 管理的典範轉變。
(D) BOVEN 試驗在 TP53 突變的 MCL 中展示 zanubrutinib + obinutuzumab + venetoclax 的療效
BOVEN 2 期試驗(2025 年報告)評估在 TP53 突變 MCL 患者中特異性評估 zanubrutinib(第二代 BTK 抑制劑)、venetoclax(BCL2 抑制劑)和 obinutuzumab(抗-CD20 抗體)的三聯組合[^10]。此高危人群通常對傳統化療的結果較差。試驗用良好耐受性的 2 年時 72% 無進展生存期和 76% 整體存活率 證明了優異結果[^10]。這代表針對此特別具有挑戰性患者亞組的重要無化療選擇。
參考文獻 (AMA)¶
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩↩↩↩↩↩↩
-
Navarro A, Clot G, Royo C, et al. Molecular Subsets of Mantle Cell Lymphoma Defined by the IGHV Mutational Status and SOX11 Expression Have Distinct Biologic and Clinical Features. Cancer Research. 2012;72(20):5307-16. doi:10.1158/0008-5472.CAN-12-1615. PMID:22915760. ↩↩↩↩↩↩
-
Fernàndez V, Salamero O, Espinet B, et al. Genomic and Gene Expression Profiling Defines Indolent Forms of Mantle Cell Lymphoma. Cancer Research. 2010;70(4):1408-18. doi:10.1158/0008-5472.CAN-09-3419. PMID:20124476. ↩↩↩↩↩↩↩↩
-
Yi S, Yan Y, Jin M, et al. Genomic and Transcriptomic Profiling Reveals Distinct Molecular Subsets Associated With Outcomes in Mantle Cell Lymphoma. The Journal of Clinical Investigation. 2022;132(3):e153283. doi:10.1172/JCI153283. PMID:34882582. ↩↩
-
Armitage JO, Longo DL. Mantle-Cell Lymphoma. The New England Journal of Medicine. 2022;386(26):2495-2506. doi:10.1056/NEJMra2202672. PMID:35767440. ↩↩
-
Jain P, Wang ML. Mantle Cell Lymphoma in 2022-a Comprehensive Update on Molecular Pathogenesis, Risk Stratification, Clinical Approach, and Current and Novel Treatments. American Journal of Hematology. 2022;97(5):638-656. doi:10.1002/ajh.26523. PMID:35266562. ↩
-
Dreyling M, Doorduijn J, Giné E, et al. Addition of Autologous Stem-Cell Transplantation to an Ibrutinib-Containing First-Line Treatment in Patients Aged 18-65 Years With Mantle Cell Lymphoma (TRIANGLE): 4·5-Year Follow-Up of a Three-Arm, Randomised, Open-Label, Phase 3 Superiority Trial of the European MCL Network. Lancet (London, England). 2026;407(10542):1953-1967. doi:10.1016/S0140-6736(26)00362-4. PMID:42134356. ↩↩↩↩↩↩
-
Dreyling M, Doorduijn J, Giné E, et al. Ibrutinib Combined With Immunochemotherapy With or Without Autologous Stem-Cell Transplantation Versus Immunochemotherapy and Autologous Stem-Cell Transplantation in Previously Untreated Patients With Mantle Cell Lymphoma (TRIANGLE): A Three-Arm, Randomised, Open-Label, Phase 3 Superiority Trial of the European Mantle Cell Lymphoma Network. Lancet (London, England). 2024;403(10441):2293-2306. doi:10.1016/S0140-6736(24)00184-3. PMID:38705160. ↩↩↩↩↩↩
-
Caserta S, Martino EA, Vigna E, et al. Bruton Tyrosine Kinase Inhibitors in Mantle Cell Lymphoma: What Are the Current Options?. European Journal of Haematology. 2025;115(6):599-609. doi:10.1111/ejh.70036. PMID:40944468. ↩↩↩↩↩↩
Figures¶