Q1. Which of the following is not high-risk cytogenetic features in multiple myeloma?¶
- (A) t(4;14)
- (B) t(14;16)
- (C) t(11;14)
- (D) t(14;20)
- (E) del(17/17p)
點此顯示正解
(C) t(11;14)
詳解¶
The correct answer is (C) t(11;14), which is NOT a high-risk cytogenetic feature in multiple myeloma. This translocation is classified as standard-risk according to the Revised International Staging System (R-ISS), Mayo Clinic mSMART risk stratification, and the 2025 International Myeloma Society/International Myeloma Working Group (IMS/IMWG) consensus criteria.146710
Why t(11;14) is Standard-Risk¶
t(11;14) is the most common IgH translocation (occurring in approximately 15-20% of newly diagnosed multiple myeloma patients) and results in overexpression of cyclin D1 through juxtaposition of the CCND1 gene on chromosome 11 with the immunoglobulin heavy chain locus on chromosome 14.[17][18][^21]
This translocation is classified as standard-risk because: - Patients with t(11;14) have a median overall survival of approximately 7-10 years, comparable to other standard-risk cytogenetic groups[17][21] - It is specifically excluded from the high-risk cytogenetic abnormalities defined in R-ISS, which only includes del(17p), t(4;14), and t(14;16)4710 - The 2025 IMS/IMWG consensus definition of high-risk myeloma does not include isolated t(11;14)1
Unique biology: t(11;14) myeloma cells exhibit BCL-2 dependence with relatively higher BCL-2 expression and lower MCL-1 expression compared to other myeloma subtypes, making them particularly sensitive to venetoclax (BCL-2 inhibitor).[^18] This has emerged as the first predictive biomarker in multiple myeloma, with venetoclax-based combinations showing response rates approaching 90% in relapsed/refractory t(11;14) patients.[18][20]
Important caveat: While t(11;14) alone is standard-risk, some recent data suggest it may confer intermediate outcomes when treated with novel agents, with slightly lower response rates and shorter progression-free survival compared to other standard-risk groups.[18][19][^20] However, it remains classified as standard-risk in all major consensus guidelines.
Why the Other Options ARE High-Risk¶

(A) t(4;14) is a high-risk cytogenetic abnormality that: - Results in overexpression of FGFR3 (fibroblast growth factor receptor 3) and MMSET genes2 - Occurs in approximately 7-8% of newly diagnosed patients2 - Is associated with worse progression-free and overall survival25 - Is included in R-ISS stage III criteria as a high-risk chromosomal abnormality4710 - In the 2025 IMS/IMWG consensus, t(4;14) is considered high-risk when co-occurring with 1q+ and/or del(1p32)1 - Median OS approximately 5-7 years (improved with bortezomib-based therapy)[17][21]
(B) t(14;16) is a high-risk cytogenetic abnormality that: - Results in overexpression of the c-MAF oncogene5 - Occurs in approximately 3-5% of newly diagnosed patients5 - Is associated with high levels of free light chains and 25% present with acute renal failure[17][21] - Is included in R-ISS stage III criteria as a high-risk chromosomal abnormality4710 - In the 2025 IMS/IMWG consensus, t(14;16) is considered high-risk when co-occurring with 1q+ and/or del(1p32)1 - Median OS approximately 3-7 years[17][21]
(D) t(14;20) is a high-risk cytogenetic abnormality that: - Results in overexpression of MAFB (MAF family transcription factor)1 - Is a rare translocation occurring in <2% of patients - Is associated with poor outcomes with median OS approximately 3-7 years[17][21] - In the 2025 IMS/IMWG consensus, t(14;20) is considered high-risk when co-occurring with 1q+ and/or del(1p32)1 - Included in high-risk IgH translocations across all major risk stratification systems125
(E) del(17p) is a high-risk cytogenetic abnormality that: - Results from loss of TP53 (tumor suppressor gene) on the short arm of chromosome 175 - Occurs in 5-20% of newly diagnosed patients5 - Is associated with significantly worse outcomes25 - Is included in R-ISS stage III criteria as a high-risk chromosomal abnormality4710 - The 2025 IMS/IMWG consensus defines high-risk as del(17p) >20% clonal fraction and/or TP53 mutation1 - Median OS approximately 3-5 years, though improved with modern therapies[17][21] - Presence of biallelic TP53 inactivation (del(17p) plus TP53 mutation) confers ultra-high-risk status5
Summary of Risk Stratification Systems¶
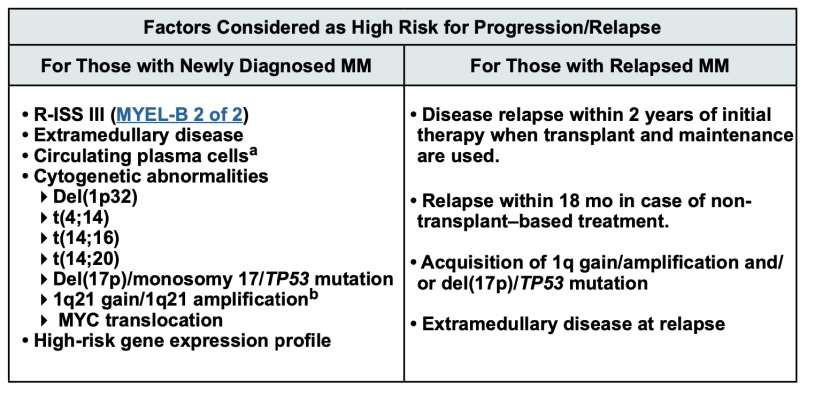
The Revised International Staging System (R-ISS) defines high-risk cytogenetic abnormalities as del(17p), t(4;14), and t(14;16) only.4710 The 2025 IMS/IMWG Consensus Genomic Staging expanded the definition to include combinations of abnormalities and specific thresholds, but t(11;14) remains excluded from high-risk criteria unless accompanied by additional high-risk features.13
詳解 · 中文翻譯¶
正確答案是 (C) t(11;14),在多發性骨髓瘤中不是高風險細胞遺傳學特徵。 此易位按修訂國際分期系統(R-ISS)、Mayo 診所 mSMART 風險分層及 2025 國際骨髓瘤學會/國際骨髓瘤工作小組(IMS/IMWG)共識標準被分類為標準風險146710。
為何 t(11;14) 是標準風險¶
t(11;14) 是最常見的 IgH 易位(發生於約 15-20% 的新診斷多發性骨髓瘤患者)且通過 11 號染色體上 CCND1 基因與 14 號染色體上免疫球蛋白重鏈基因位點並置導致 cyclin D1 過度表達[17][18][^21]。
此易位被分類為標準風險因為: - 具有 t(11;14) 的患者有中位整體存活約 7-10 年,與其他標準風險細胞遺傳學群組相當[17][21] - 它 明確被排除於在 R-ISS 中定義的高風險細胞遺傳學異常,僅包括 del(17p)、t(4;14) 及 t(14;16)4710 - 2025 IMS/IMWG 高風險骨髓瘤的共識定義 不包括單獨的 t(11;14)1
獨特生物學:t(11;14) 骨髓瘤細胞展現 BCL-2 相依性,BCL-2 表達相對更高、MCL-1 表達較低相比其他骨髓瘤亞型,使其特別 對 venetoclax(BCL-2 抑制劑)敏感[^18]。此已出現為多發性骨髓瘤中的第一個預測性生物標誌物,venetoclax 基礎合併療法在復發/難治 t(11;14) 患者中顯示應答率接近 90%[18][20]。
重要警告:雖然 t(11;14) 單獨為標準風險,某些最近資料提示它可能賦予中等預後當用新型藥物治療時,應答率略低、無進展存活期較短相比其他標準風險群組[18][19][^20]。然而,它在所有主要共識指南中仍被分類為標準風險。
為何其他選項是高風險¶
(A) t(4;14) 是一個 高風險細胞遺傳學異常,該: - 導致 FGFR3(纖維母細胞生長因子受體 3)和 MMSET 基因過度表達2 - 發生於約 7-8% 的新診斷患者2 - 與 更差的無進展及整體存活相關聯25 - 在 R-ISS III 期標準中作為高風險染色體異常被納入4710 - 在 2025 IMS/IMWG 共識中,t(4;14) 被認為高風險 當合併 1q+ 及/或 del(1p32) 時1 - 中位 OS 約 5-7 年(用 bortezomib 基礎治療改善)[17][21]
(B) t(14;16) 是一個 高風險細胞遺傳學異常,該: - 導致 c-MAF 癌基因過度表達5 - 發生於約 3-5% 的新診斷患者5 - 與 高水準遊離輕鏈相關聯且 25% 現況有急性腎衰竭[17][21] - 在 R-ISS III 期標準中作為高風險染色體異常被納入4710 - 在 2025 IMS/IMWG 共識中,t(14;16) 被認為高風險 當合併 1q+ 及/或 del(1p32) 時1 - 中位 OS 約 3-7 年[17][21]
(D) t(14;20) 是一個 高風險細胞遺傳學異常,該: - 導致 MAFB(MAF 族轉錄因子)過度表達1 - 是一個 罕見易位,發生於 <2% 的患者 - 與 預後不佳相關聯,中位 OS 約 3-7 年[17][21] - 在 2025 IMS/IMWG 共識中,t(14;20) 被認為高風險 當合併 1q+ 及/或 del(1p32) 時1 - 在所有主要風險分層系統中被納入高風險 IgH 易位125
(E) del(17p) 是一個 高風險細胞遺傳學異常,該: - 源於 TP53(腫瘤抑制基因)在 17 號染色體短臂上的喪失5 - 發生於 5-20% 的新診斷患者5 - 與 明顯更差的預後相關聯25 - 在 R-ISS III 期標準中作為高風險染色體異常被納入4710 - 2025 IMS/IMWG 共識定義高風險為 del(17p) >20% 克隆分數及/或 TP53 突變1 - 中位 OS 約 3-5 年,雖然用現代治療改善[17][21] - 雙等位 TP53 失活的存在(del(17p) 加 TP53 突變)賦予超高風險狀態5
風險分層系統總結¶
修訂國際分期系統(R-ISS) 定義高風險細胞遺傳學異常為 del(17p)、t(4;14) 及 t(14;16) 僅有4710。2025 IMS/IMWG 共識基因組分期擴展了定義以納入異常組合及特定閾值,但 t(11;14) 仍被排除於高風險標準除非伴隨額外高風險特徵13。
參考文獻 (AMA)¶
-
Avet-Loiseau H, Davies FE, Samur MK, et al. International Myeloma Society/International Myeloma Working Group Consensus Recommendations on the Definition of High-Risk Multiple Myeloma. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2025;:JCO2401893. doi:10.1200/JCO-24-01893. PMID:40489728. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(14):1228-1263. doi:10.1200/JCO.18.02096. PMID:30932732. ↩↩↩↩↩↩↩↩↩↩
-
National Comprehensive Cancer Network. Multiple Myeloma. https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf#page=17. ↩↩
-
Rajkumar SV. Multiple Myeloma: 2022 Update on Diagnosis, Risk Stratification, and Management. American Journal of Hematology. 2022;97(8):1086-1107. doi:10.1002/ajh.26590. PMID:35560063. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Rajkumar SV. Multiple Myeloma: 2024 Update on Diagnosis, Risk-Stratification, and Management. American Journal of Hematology. 2024;99(9):1802-1824. doi:10.1002/ajh.27422. PMID:38943315. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Paner A, Patel P, Dhakal B. The Evolving Role of Translocation T(11;14) in the Biology, Prognosis, and Management of Multiple Myeloma. Blood Reviews. 2020;41:100643. doi:10.1016/j.blre.2019.100643. PMID:31818702. ↩↩
-
J Clin Oncol 40, 2022 (suppl 16; abstr 8064). https://meetings.asco.org/abstracts-presentations/207915. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Saini N, Ma J, Milton DR, et al. Impact of Autologous Transplantation in Patients With Multiple Myeloma With T(11;14): A Propensity-Score Matched Analysis. Clinical Cancer Research : An Official Journal of the American Association for Cancer Research. 2019;25(22):6781-6787. doi:10.1158/1078-0432.CCR-19-0706. PMID:31481508. ↩
-
Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and Management of Multiple Myeloma: A Review. Jama. 2022;327(5):464-477. doi:10.1001/jama.2022.0003. PMID:35103762. ↩
-
Schavgoulidze A, Perrot A, Leleu X, et al. High-Risk Genomic Consensus Validation for Patients With Newly Diagnosed Multiple Myeloma Using Next-Generation Sequencing. Blood. 2026;147(3):266-275. doi:10.1182/blood.2025029999. PMID:40991836. ↩↩↩↩↩↩↩↩↩↩↩↩
Slide annotations
The table provides a list of high-risk cytogenetic features for multiple myeloma, which includes t(4;14), t(14;16), t(14;20), and del(17p), but excludes t(11;14).
Figures¶