Q1. Which of the following is (are) immune-privileged large B cell lymphoma defined by WHO 5th classification? (1) Primary DLBCL of CNS (2) Retinovitreal DLBCL (3) Testicular DLBCL (4) Adrenal DLBCL¶
- (A) 1
- (B) 1+3
- (C) 2+4
- (D) 1+2+3
- (E) 1+2+3+4
點此顯示正解
(D) 1+2+3
詳解¶
1. Why (D) is correct per WHO-5 classification¶
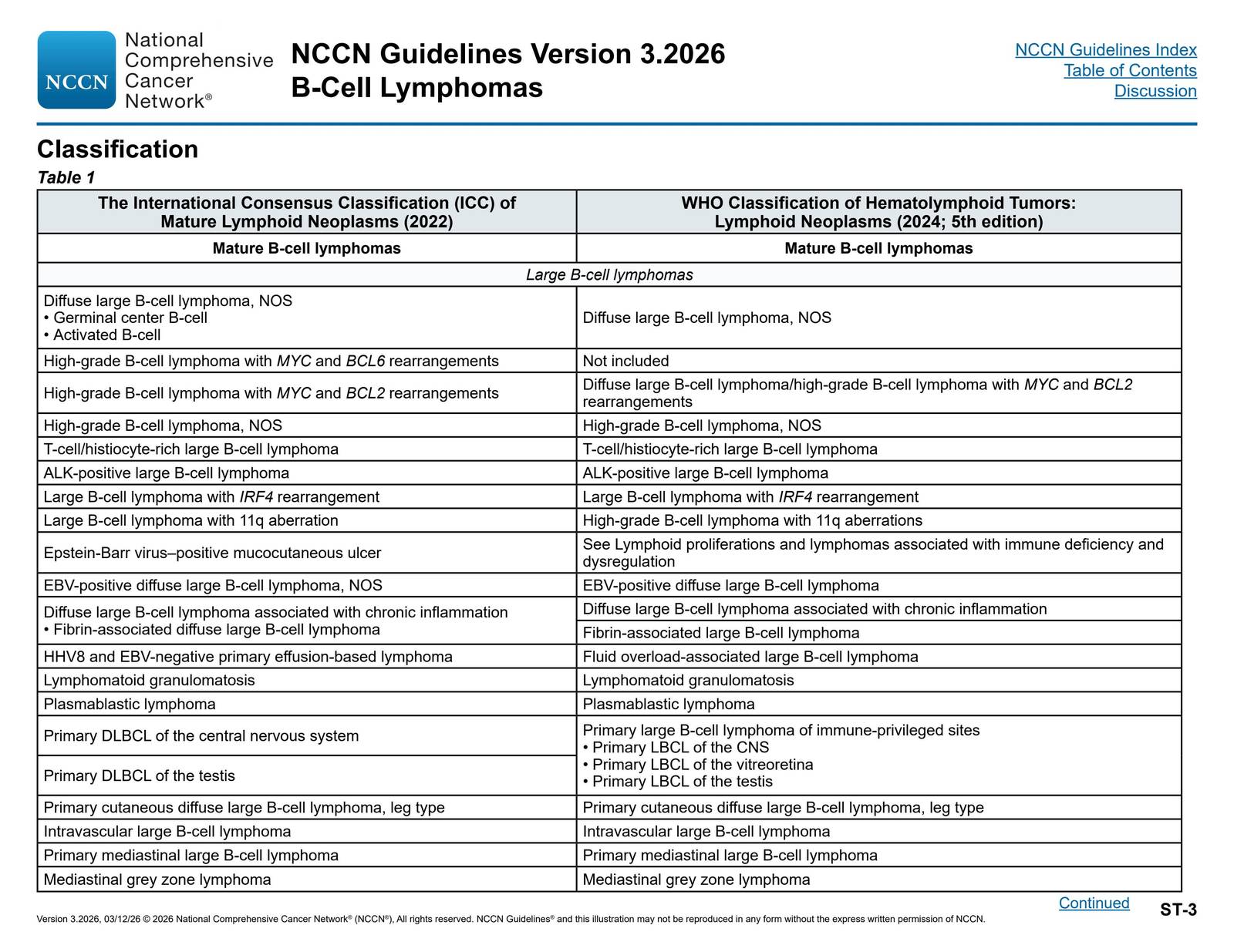
The WHO 5th edition classification defines primary large B-cell lymphoma of immune-privileged sites (IP-LBCL) as a distinct entity encompassing three specific anatomic sites: (1) primary LBCL of the CNS, (2) primary LBCL of the vitreoretina, and (3) primary LBCL of the testis1235. This classification reflects the recognition that lymphomas arising in these anatomically and immunologically privileged sites share distinctive clinical, pathologic, and molecular features.
The NCCN guidelines comparison table between the ICC and WHO-5 classifications explicitly shows this grouping:
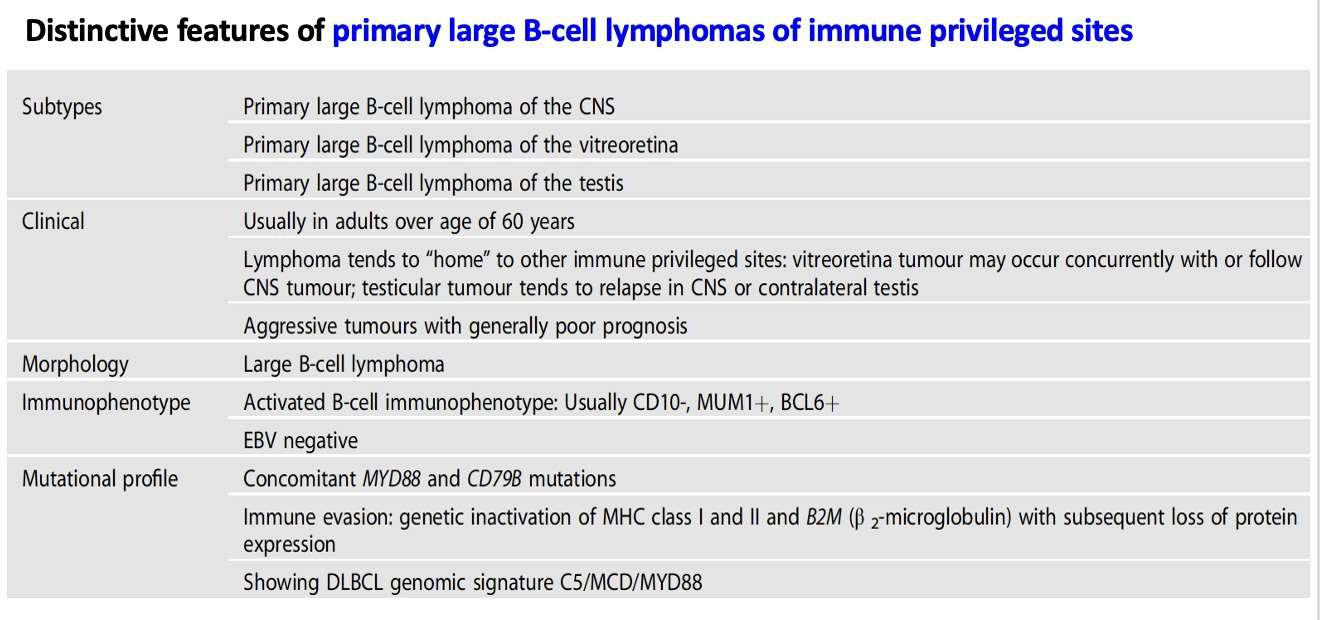
These three entities share key biological characteristics that justify their unified classification1[^8]:
Molecular features: Predominantly activated B-cell (ABC) immunophenotype with frequent co-mutations of MYD88 (L265P) and CD79B, characteristic of the MCD/C5/MYD88 genetic subtype. Frequent genetic alterations promoting immune evasion, including loss of HLA class I/II expression1[^8].
Clinical behavior: Strong predilection for remaining confined to extranodal sites, marked CNS tropism, and tendency to arise within anatomic sanctuary sites with limited immune surveillance1[^8].
Immunophenotype: Typically CD10-/BCL6+/MUM1+ pattern consistent with ABC origin1[^7].
2. Why adrenal DLBCL is NOT classified as immune-privileged in WHO-5¶
Despite sharing some molecular similarities with IP-LBCL, adrenal DLBCL is NOT included in the WHO-5 immune-privileged site category[^8]. The key distinction is that the adrenal gland is not considered an immune-privileged site from an anatomic or immunologic standpoint[^8].
While primary adrenal large B-cell lymphoma (PA-LBCL) exhibits overlapping features with IP-LBCL—including similar immunophenotype (CD10-/BCL6+/MUM1+), frequent PIM1, MYD88 L265P, and CD79B mutations[^7]—it demonstrates greater genomic heterogeneity compared to the three recognized IP-LBCL sites[^8]. As noted in a comprehensive review: "Other extranodal DLBCL involving the breast, adrenal glands, and skin are often ABC DLBCL but are more heterogeneous in their genomic profile and involve anatomic sites that are not considered immune privileged"[^8].
Recent molecular studies suggest PA-LBCL may warrant future consideration for inclusion in IP-LBCL based on shared clinical features and molecular profiles[^7], but this has not been incorporated into the current WHO-5 classification. The adrenal gland lacks the specialized immune-privileged microenvironment characteristic of the CNS, vitreoretina, and testis, which have unique blood-tissue barriers and limited immune surveillance mechanisms[^11].
詳解 · 中文翻譯¶
1. 為何 (D) 根據 WHO-5 分類是正確的¶
WHO 第 5 版分類 定義 免疫特權部位原發性大 B 細胞淋巴瘤(IP-LBCL) 為一個明確實體,涵蓋 三個特定解剖位點:(1) 中樞神經系統原發性淋巴瘤、(2) 玻璃體視網膜原發性淋巴瘤和 (3) 睾丸原發性淋巴瘤1235。此分類反映了在這些解剖上和免疫上特權位點發生的淋巴瘤共享獨特臨床、病理和分子特徵的認識。
NCCN 指南在 ICC 和 WHO-5 分類之間的比較表明確顯示此分組:
這三個實體共享可以證實其統一分類的關鍵生物特徵1[^8]:
分子特徵:主要活化 B 細胞(ABC)免疫表型,頻繁 MYD88(L265P)和 CD79B 共突變,MCD/C5/MYD88 遺傳亞型的特徵。促進免疫逃避的頻繁遺傳改變,包括 HLA 第一類/二類表達喪失1[^8]。
臨床行為:強烈的傾向保持在結外位點,明顯的中樞神經系統親和力,和傾向於在免疫監視有限的解剖聖域位點中發生1[^8]。
免疫表型:通常 CD10-/BCL6+/MUM1+ 模式符合 ABC 來源1[^7]。
2. 為何腎上腺 DLBCL 在 WHO-5 中未分類為免疫特權¶
儘管與 IP-LBCL 共享一些分子相似性,腎上腺 DLBCL 不包含在 WHO-5 免疫特權位點類別中[^8]。關鍵區別是 腎上腺腺體從解剖或免疫學角度不被認為是免疫特權位點[^8]。
雖然原發性腎上腺大 B 細胞淋巴瘤(PA-LBCL)表現出與 IP-LBCL 重疊的特徵——包括相似的免疫表型(CD10-/BCL6+/MUM1+)、頻繁的 PIM1、MYD88 L265P 和 CD79B 突變[^7]——它相比三個公認的 IP-LBCL 位點顯示 更大的基因組異質性[^8]。如一項全面評論中所述:「涉及乳房、腎上腺和皮膚的其他結外 DLBCL 通常是 ABC DLBCL,但在其基因組譜中更加異質,涉及不被認為免疫特權的解剖位點」[^8]。
最近的分子研究表明 PA-LBCL 可能值得基於共享臨床特徵和分子譜將來考慮納入 IP-LBCL[^7],但這尚未納入當前 WHO-5 分類。腎上腺腺體缺乏中樞神經系統、玻璃體視網膜和睾丸特有的專業免疫特權微環境,這些具有獨特的血液-組織屏障和有限的免疫監視機制[^11]。
參考文獻 (AMA)¶
-
Roschewski M, Phelan JD, Jaffe ES. Primary Large B-Cell Lymphomas of Immune-Privileged Sites. Blood. 2024;144(25):2593-2603. doi:10.1182/blood.2023020911. PMID:38635786. ↩↩↩↩↩↩↩↩↩↩
-
Wang H, Zhang Y, Wan X, Li Z, Bai O. In the Era of Targeted Therapy and Immunotherapy: Advances in the Treatment of Large B-Cell Lymphoma of Immune-Privileged Sites. Frontiers in Immunology. 2025;16:1547377. doi:10.3389/fimmu.2025.1547377. PMID:40292282. ↩↩
-
Wang L, Guo M, Hou S. Advances in Primary Large B-Cell Lymphoma of Immune-Privileged Sites. Frontiers in Immunology. 2025;16:1533444. doi:10.3389/fimmu.2025.1533444. PMID:40078990. ↩↩
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=134. ↩
-
Deng S, Li A, Wang Z, et al. Clinicopathological, Genomic, and Transcriptomic Feature Analysis of Primary Adrenal Large B-Cell Lymphoma: Insights Into Immune-Privileged Sites. The American Journal of Surgical Pathology. 2025;:00000478-990000000-00537. doi:10.1097/PAS.0000000000002426. PMID:40485393. ↩↩
-
Takahara T, Nakamura S, Tsuzuki T, Satou A. The Immunology of DLBCL. Cancers. 2023;15(3):835. doi:10.3390/cancers15030835. PMID:36765793. ↩
Slide annotations
Table provided describing distinctive features of primary large B-cell lymphomas of immune privileged sites.
Figures¶