According to an invited review in the New England Journal of Medicine, this clinical presentation is highly suggestive of **hemophagocytic lymphohistiocytosis (HLH)**, and all four diagnostic and management steps outlined in the board question are appropriate[^1][^3].
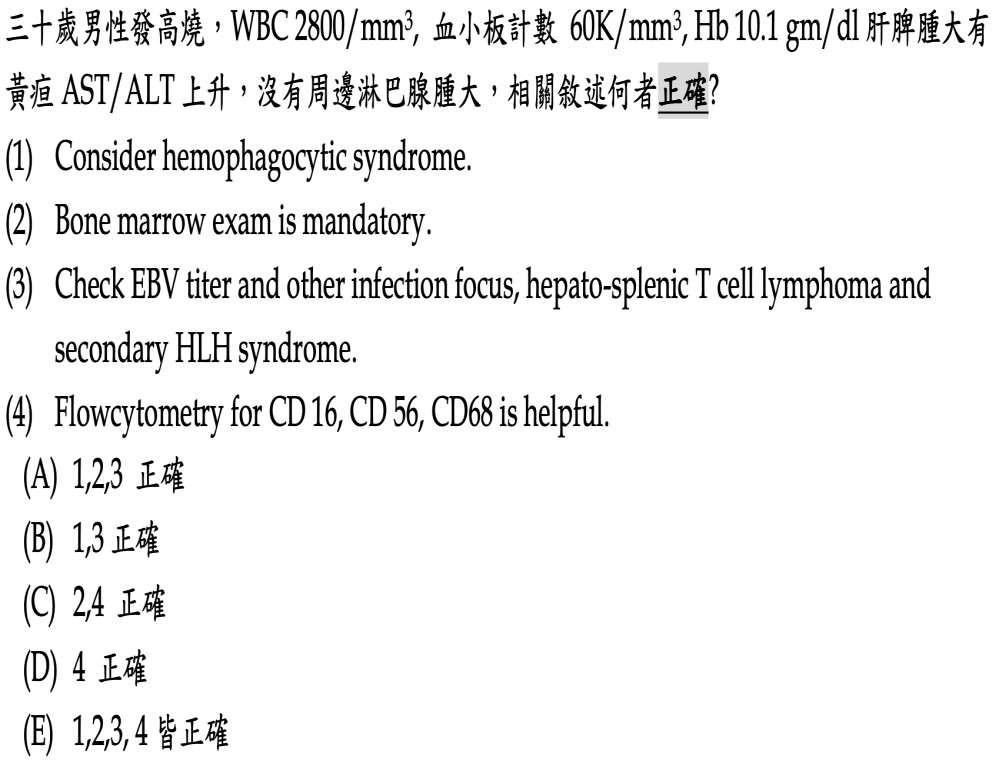
**Statement 1: Consider hemophagocytic syndrome (HLH)** is correct. The patient meets multiple HLH-2004 diagnostic criteria: **fever** (≥38.5°C), **splenomegaly**, **bicytopenia** (WBC 2800/mm³ with neutropenia likely, platelets 60,000/mm³, hemoglobin 10.1 g/dL), and **hepatitis** (elevated AST/ALT with hepatomegaly and jaundice)[^1][^4]. The HLH-2004 criteria require five of eight features for diagnosis: fever, splenomegaly, bicytopenia affecting at least two lineages, hypertriglyceridemia or hypofibrinogenemia, hemophagocytosis, hyperferritinemia (≥500 μg/L), low or absent NK-cell activity, and elevated soluble CD25 (≥2400 U/mL)[^1][^4]. This patient already demonstrates at least four criteria clinically, making HLH a leading diagnostic consideration. Though hepatitis is not part of the formal diagnostic criteria, it is **extremely common in HLH** and supports the diagnosis[^1].
**Statement 2: Bone marrow exam is mandatory** is correct. Bone marrow biopsy serves multiple critical purposes in suspected HLH: it can identify **hemophagocytosis** (one of the HLH-2004 diagnostic criteria), rule out **underlying hematologic malignancy** (a common trigger of secondary HLH), and assess for cytopenias and histiocyte hyperplasia[^1][^3]. The review emphasizes that prompt diagnosis is essential to reduce mortality and morbidity, particularly neurologic complications, and bone marrow examination is a key component of the diagnostic workup[^1].
**Statement 3: Check EBV titer and other infection focus, hepatosplenic T-cell lymphoma, and secondary HLH syndrome** is correct. The review stresses that **a meticulous search for the underlying triggering factor should be continued in all patients**, including those receiving ongoing HLH treatment[^3]. Epstein-Barr virus (EBV) is a well-recognized trigger of secondary HLH, particularly in young adults. Hepatosplenic T-cell lymphoma is a rare but important malignancy-associated trigger that can present with hepatosplenomegaly, cytopenias, and no peripheral lymphadenopathy—matching this patient's presentation. The absence of peripheral lymphadenopathy is notable, as **adenopathy is not common in HLH and may suggest underlying lymphoma** when present[^3].
**Statement 4: Flow cytometry for CD16, CD56, CD68 is helpful** is correct. Flow cytometry serves dual diagnostic purposes in this scenario. **CD16 and CD56** are natural killer (NK) cell markers; NK-cell activity assessment can fulfill one of the HLH-2004 diagnostic criteria (low or absent NK-cell activity)[^1][^4]. Additionally, flow cytometry is crucial for identifying underlying lymphoma: hepatosplenic T-cell lymphoma typically shows a **CD3+, CD4-, CD8-/+, CD56+/-** immunophenotype. **CD68** is a macrophage/histiocyte marker that can help identify the activated histiocyte population characteristic of HLH and may reveal hemophagocytosis on bone marrow or tissue samples[^1]. Flow cytometry is also essential for detecting cytopenias and histiocyte hyperplasia, providing additional diagnostic clues for HLH[^1].
Additional context from diagnostic guidelines: The North American Consortium for Histiocytosis (NACHO) recommendations reinforce that bone marrow biopsy is essential to rule out malignancy, identify hemophagocytosis, and identify CNS involvement[6][8]. The essential workup for suspected HLH includes cultures and viral PCRs for EBV, CMV, and adenovirus to search for triggering infections[6][8]. Body cavity imaging (chest/abdomen/pelvis CT) should be routinely performed to help rule out malignancy or unusual infections, with PET-CT being particularly helpful for guiding biopsy if lymphoma is suspected[6][8].
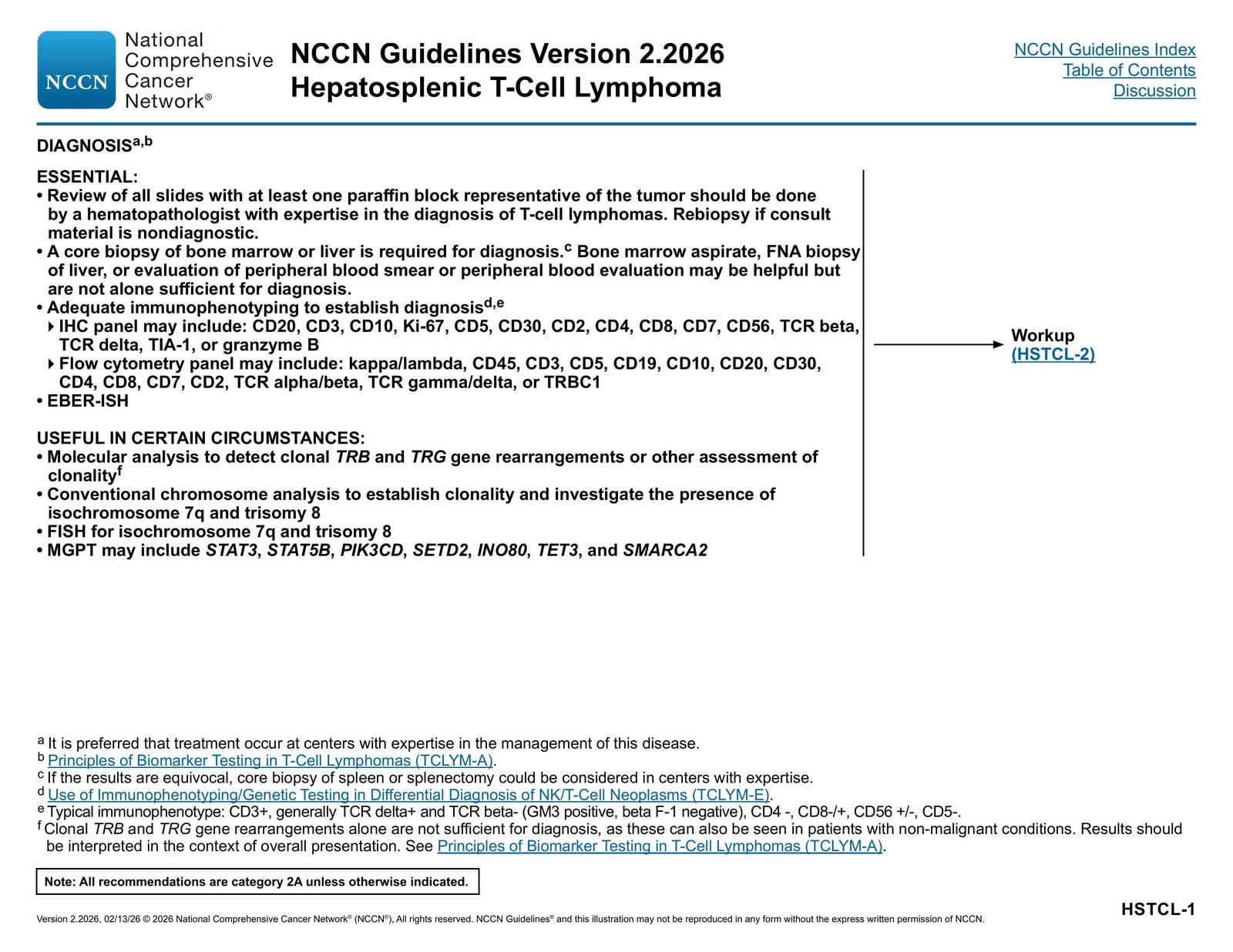
Hepatosplenic T-cell lymphoma considerations: NCCN guidelines specify that hepatosplenic T-cell lymphoma diagnosis requires core biopsy of bone marrow or liver by a hematopathologist with expertise in T-cell lymphomas[^9]. The typical immunophenotype is CD3+, generally TCR delta+ and TCR beta-, CD4-, CD8-/+, CD56+/-, CD5-[^9]. Flow cytometry panels should include CD56 (an NK-cell marker that can be positive in this lymphoma), and immunohistochemistry may include CD56 and CD68 among other markers[^9]. This lymphoma can trigger secondary HLH, making the distinction between primary lymphoma and HLH-associated findings critical.
In summary, this 30-year-old man with fever, pancytopenia, hepatosplenomegaly, hepatitis, and no peripheral adenopathy requires urgent evaluation for HLH with simultaneous investigation for underlying triggers, particularly EBV infection and hepatosplenic T-cell lymphoma. All four statements represent appropriate and complementary diagnostic steps that should be pursued concurrently to establish the diagnosis and identify treatable underlying causes.
Henter JI. Hemophagocytic Lymphohistiocytosis. The New England Journal of Medicine. 2025;392(6):584-598. doi:10.1056/NEJMra2314005. PMID:39908433. ↩
Jordan MB, Allen CE, Greenberg J, et al. Challenges in the Diagnosis of Hemophagocytic Lymphohistiocytosis: Recommendations From the North American Consortium for Histiocytosis (NACHO). Pediatric Blood & Cancer. 2019;66(11):e27929. doi:10.1002/pbc.27929. PMID:31339233. ↩
Jordan MB, Allen CE, Greenberg J, et al. Challenges in the Diagnosis of Hemophagocytic Lymphohistiocytosis: Recommendations From the North American Consortium for Histiocytosis (NACHO). Pediatric Blood & Cancer. 2019;66(11):e27929. doi:10.1002/pbc.27929. PMID:31339233. ↩
National Comprehensive Cancer Network. T-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/t-cell.pdf#page=49. ↩