Q53. Which of the following findings are considered as high risk FISH features defined by multiple myeloma R-ISS? (1) t(4;14). (2) t(6;14). (3) t(14;16). (4) Del13q. (5) Del17p.¶
- (A) 1+2+4
- (B) 1+2+5
- (C) 1+3+5
- (D) 2+3+4
- (E) 2+3+5
點此顯示正解
(C) 1+3+5
詳解¶
The correct answer is (C) 1+3+5, which includes t(4;14), t(14;16), and del(17p) — the three high-risk FISH abnormalities specifically defined by the R-ISS for multiple myeloma.45
Why (C) Matches R-ISS High-Risk FISH Criteria¶
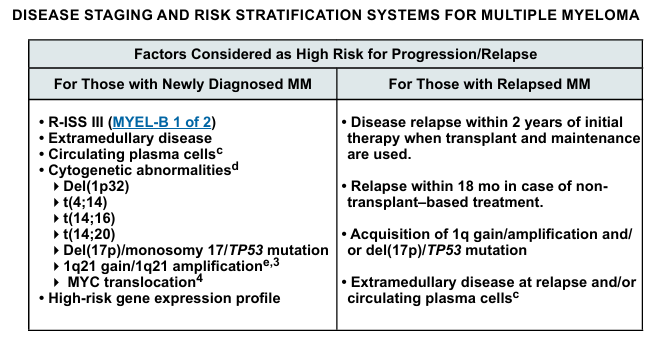
The Revised International Staging System (R-ISS), published by Palumbo et al. in 2015, explicitly defines high-risk chromosomal abnormalities (CA) as del(17p), t(4;14), and t(14;16) detected by interphase FISH after CD138 plasma cell purification.5 These three abnormalities are incorporated into R-ISS staging as follows:
- R-ISS Stage I: ISS stage I with normal LDH and standard-risk CA (absence of the three high-risk abnormalities)
- R-ISS Stage III: ISS stage III (β2-microglobulin ≥5.5 mg/L) with high LDH and/or high-risk CA [del(17p), t(4;14), or t(14;16)]
- R-ISS Stage II: All other combinations45
In the original R-ISS cohort of 3,060 patients, 5-year overall survival rates were 82% for R-ISS I, 62% for R-ISS II, and 40% for R-ISS III, demonstrating the prognostic power of this classification.5
Why t(6;14) and del(13q) Are NOT R-ISS High-Risk¶
t(6;14) is classified as a standard-risk IgH translocation in multiple myeloma risk stratification systems. The Mayo Clinic mSMART classification explicitly lists t(6;14) under standard-risk abnormalities, along with trisomies and t(11;14), distinguishing it from high-risk IgH translocations such as t(4;14), t(14;16), and t(14;20).[11][12]
del(13q) detected by FISH is not included in R-ISS high-risk criteria. While del(13q) was historically associated with poor prognosis when detected by conventional cytogenetics, multivariate analyses in the modern era have shown that its adverse prognostic significance is largely explained by its association with other high-risk abnormalities, particularly t(4;14) and del(17p). When these factors are accounted for in contemporary risk models like R-ISS, del(13q) by FISH alone does not independently define high-risk disease.5
Contemporary Context¶
While the R-ISS remains the standard for routine clinical practice, recent consensus recommendations from the International Myeloma Society/International Myeloma Working Group (2025) have proposed an updated Consensus Genomic Staging (CGS) that incorporates additional high-risk features including 1q gain/amplification, del(1p32), and t(14;20), reflecting evolving understanding of myeloma biology in the era of modern therapies.2 However, for the specific question about R-ISS-defined high-risk FISH features, the answer remains t(4;14), t(14;16), and del(17p).
詳解 · 中文翻譯¶
正確答案是 (C) 1+3+5,包括 t(4;14)、t(14;16) 和 del(17p) — R-ISS 特別定義的三個高危 FISH 異常。45
為什麼 (C) 符合 R-ISS 高危 FISH 標準¶
由 Palumbo 等人在 2015 年發表的修訂國際分期系統 (R-ISS) 明確定義高危染色體異常 (CA) 為 del(17p)、t(4;14) 和 t(14;16),通過 CD138 漿細胞淨化後的間期 FISH 檢測。5 這三個異常被納入 R-ISS 分期如下:
- R-ISS 1 期:ISS 1 期,正常 LDH 和標準風險 CA(缺乏三個高危異常)
- R-ISS 3 期:ISS 3 期(β2 微球蛋白 ≥5.5 mg/L)具有高 LDH 和/或高危 CA [del(17p)、t(4;14) 或 t(14;16)]
- R-ISS 2 期:所有其他組合45
在原始 R-ISS 3,060 患者隊列中,5 年整體存活率為 R-ISS I 的 82%、R-ISS II 的 62% 和 R-ISS III 的 40%,展示此分類的預後能力。5
為什麼 t(6;14) 和 del(13q) 不是 R-ISS 高危¶
t(6;14) 被分類為多發性骨髓瘤風險分層系統中的標準風險 IgH 易位。Mayo 診所 mSMART 分類明確將 t(6;14) 列在標準風險異常下,與三體和 t(11;14) 一起,區別於高危 IgH 易位如 t(4;14)、t(14;16) 和 t(14;20)。[11][12]
FISH 檢測的 del(13q) 不包括在 R-ISS 高危標準中。雖然 del(13q) 在用常規細胞遺傳學檢測時歷史上與差預後相關,現代時代的多變量分析表明其不利預後顯著性主要由其與其他高危異常的關聯解釋,特別是 t(4;14) 和 del(17p)。當這些因素在當代風險模型如 R-ISS 中考慮時,FISH 檢測的 del(13q) 單獨不獨立定義高危疾病。5
當代背景¶
雖然 R-ISS 仍然是常規臨床實踐的標準,來自國際骨髓瘤協會/國際骨髓瘤工作組(2025)的最近共識建議提出更新的共識基因組分期 (CGS),納入其他高危特徵,包括 1q 增益/擴增、del(1p32) 和 t(14;20),反映現代療法時代對骨髓瘤生物學的不斷演進的理解。2 然而,對於關於 R-ISS 定義的高危 FISH 特徵的特定問題,答案仍然是 t(4;14)、t(14;16) 和 del(17p)。
參考文獻 (AMA)¶
-
Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(14):1228-1263. doi:10.1200/JCO.18.02096. PMID:30932732. ↩
-
Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2015;33(26):2863-9. doi:10.1200/JCO.2015.61.2267. PMID:26240224. ↩↩
-
Rajkumar SV. Multiple Myeloma: 2020 Update on Diagnosis, Risk-Stratification and Management. American Journal of Hematology. 2020;95(5):548-567. doi:10.1002/ajh.25791. PMID:32212178. ↩
-
Rajkumar SV. Multiple Myeloma: 2022 Update on Diagnosis, Risk Stratification, and Management. American Journal of Hematology. 2022;97(8):1086-1107. doi:10.1002/ajh.26590. PMID:35560063. ↩↩↩↩
-
Avet-Loiseau H, Davies FE, Samur MK, et al. International Myeloma Society/International Myeloma Working Group Consensus Recommendations on the Definition of High-Risk Multiple Myeloma. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2025;:JCO2401893. doi:10.1200/JCO-24-01893. PMID:40489728. ↩↩↩↩↩↩↩↩↩↩
Slide annotations
Table on the right provides additional context for high-risk features in multiple myeloma.
Figures¶