Q1. Which criteria is not the recommended criteria for high-risk smoldering multiple myeloma (SMM)?¶
- (A) Serum M protein ≥ 3g/dL.
- (B) IgG SMM.
- (C) Bone marrow plasma cell 50-60%.
- (D) t(4;14) or del 17p or 1q gain.
- (E) Positron emission tomography-computed tomography (PET/CT) with focal lesion with increased uptake without underlying osteolytic bone destruction.
點此顯示正解
(B) IgG SMM.
詳解¶
The correct answer is (B) IgG SMM — immunoglobulin isotype (IgG) is NOT a recognized high-risk criterion for smoldering multiple myeloma according to established risk stratification models.
Why IgG SMM is NOT a high-risk criterion:
The Mayo 2018 criteria and IMWG risk models for high-risk SMM do not include immunoglobulin isotype as a risk factor234. While IgA isotype has been associated with modestly increased progression risk compared to IgG in some studies of MGUS (adjusted OR 1.80)[^7] and was identified as a risk factor in earlier SMM cohorts[^9], isotype alone is not incorporated into current validated high-risk SMM criteria. The established risk models focus on quantitative markers (M-protein level, bone marrow plasma cell percentage, FLC ratio) and specific high-risk features (cytogenetics, imaging findings), not on whether the monoclonal protein is IgG versus IgA234.
Why the other options ARE recognized high-risk SMM features:
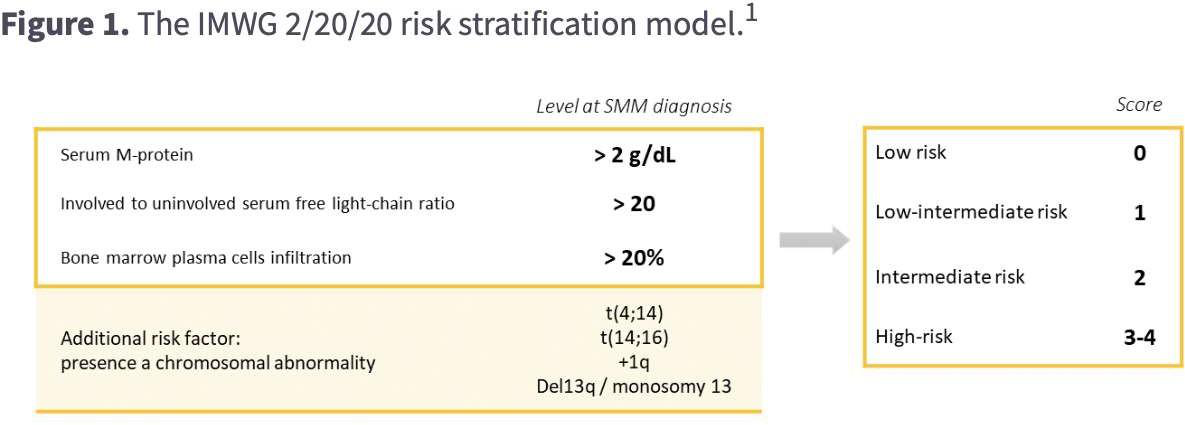
(A) Serum M-protein ≥3 g/dL: This exceeds the >2 g/dL threshold in the Mayo 2018 "2/20/20" model, which defines high-risk SMM as having 2-3 of the following: serum M-protein >2 g/dL, bone marrow plasma cells >20%, or FLC ratio >20234.
(C) Bone marrow plasma cells 50-60%: This is explicitly listed as a high-risk feature in the Mayo criteria. While ≥60% bone marrow plasma cells now meets the revised IMWG definition of active multiple myeloma, 50-60% remains within the SMM range and represents a very high-risk subset with rapid progression234.
(D) High-risk cytogenetics (t(4;14), del17p, 1q gain): These specific cytogenetic abnormalities are recognized high-risk factors for SMM progression and are listed in the Mayo criteria as "other high-risk factors"234.
(E) PET-CT focal lesion without osteolytic destruction: This imaging finding is specifically included in the Mayo criteria as a high-risk feature. It represents focal disease activity that has not yet caused bone destruction (which would meet myeloma-defining events)234.
詳解 · 中文翻譯¶
正確答案是 (B) IgG 悶燒多發性骨髓瘤 — 免疫球蛋白同型(IgG)不是公認的悶燒多發性骨髓瘤高風險標準,根據既定風險分層模型。
為何 IgG 悶燒多發性骨髓瘤不是高風險標準:
Mayo 2018 標準和 IMWG 悶燒多發性骨髓瘤高風險模型不包括免疫球蛋白同型作為風險因素234。雖然 IgA 同型在一些 MGUS 研究中已與相比 IgG 的適度增加進展風險相關(調整後 OR 1.80)[7],並在早期悶燒多發性骨髓瘤隊列中被識別為風險因素[9],同型單獨不被納入當前驗證的高風險悶燒多發性骨髓瘤標準。既定風險模型集中於定量標誌物(M-蛋白水平、骨髓漿細胞百分比、FLC 比率)和特定高風險特徵(細胞遺傳學、影像發現),而非單克隆蛋白是 IgG 還是 IgA234。
為何其他選項是公認的高風險悶燒多發性骨髓瘤特徵:
(A) 血清 M-蛋白 ≥3 g/dL: 這超過 Mayo 2018「2/20/20」模型中的 >2 g/dL 閾值,定義高風險悶燒多發性骨髓瘤為具有以下 2-3 項:血清 M-蛋白 >2 g/dL、骨髓漿細胞 >20% 或 FLC 比率 >20234。
(C) 骨髓漿細胞 50-60%: 這在 Mayo 標準中明確列為高風險特徵。雖然 ≥60% 骨髓漿細胞現在符合修訂的 IMWG 活動性多發性骨髓瘤定義,50-60% 仍在悶燒多發性骨髓瘤範圍內,代表進展迅速的非常高風險子集234。
(D) 高風險細胞遺傳學(t(4;14)、del17p、1q 獲得): 這些特定細胞遺傳學異常是公認的悶燒多發性骨髓瘤進展高風險因素,在 Mayo 標準中作為「其他高風險因素」列出234。
(E) PET-CT 焦點病變無骨溶解破壞: 此影像發現在 Mayo 標準中明確包含為高風險特徵。它代表尚未引起骨破壞的焦點疾病活性(將符合骨髓瘤定義事件)234。
參考文獻 (AMA)¶
-
Rajkumar SV. Multiple Myeloma: 2022 Update on Diagnosis, Risk Stratification, and Management. American Journal of Hematology. 2022;97(8):1086-1107. doi:10.1002/ajh.26590. PMID:35560063. ↩
-
Rajkumar SV. Multiple Myeloma: 2024 Update on Diagnosis, Risk-Stratification, and Management. American Journal of Hematology. 2024;99(9):1802-1824. doi:10.1002/ajh.27422. PMID:38943315. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Rajkumar SV. Multiple Myeloma: 2020 Update on Diagnosis, Risk-Stratification and Management. American Journal of Hematology. 2020;95(5):548-567. doi:10.1002/ajh.25791. PMID:32212178. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Landgren O, Hofmann JN, McShane CM, et al. Association of Immune Marker Changes With Progression of Monoclonal Gammopathy of Undetermined Significance to Multiple Myeloma. JAMA Oncology. 2019;5(9):1293-1301. doi:10.1001/jamaoncol.2019.1568. PMID:31318385. ↩↩↩↩↩↩↩↩↩↩↩↩
-
Kyle RA, Remstein ED, Therneau TM, et al. Clinical Course and Prognosis of Smoldering (Asymptomatic) Multiple Myeloma. The New England Journal of Medicine. 2007;356(25):2582-90. doi:10.1056/NEJMoa070389. PMID:17582068. ↩
Slide annotations
Figure 1. The IMWG 2/20/20 risk stratification model.
Figures¶