Q1. 一位 70 歲男性有明顯可摸到的脾臟腫大,PB 邊邊血中 WBC:15,000/mm³, lymphocyte 45%, villous lymphocyte,身體其他部位摸不到淋巴腺腫大,輕微貧血,血小板計數正常。flowcytometry 顯示 CD5-, CD20+, CD10-, CD43-, BCL2+, bone marrow lymphocyte >40%。最合適的診斷為何?¶
- (A) Mantle cell lymphoma
- (B) Hairy cell leukemia
- (C) Splenic marginal zone lymphoma
- (D) Splenic follicular lymphoma
- (E) Hepatosplenic lymphoma
點此顯示正解
(C) Splenic marginal zone lymphoma
詳解¶
1. Why (C) Splenic Marginal Zone Lymphoma is Correct¶
Splenic marginal zone lymphoma (SMZL) is the most likely diagnosis based on the constellation of splenomegaly without peripheral lymphadenopathy, villous lymphocytes in peripheral blood, and the characteristic CD5-/CD20+/CD10-/CD43-/BCL2+ immunophenotype123.
Villous lymphocytes are a hallmark morphologic feature of SMZL. These cells appear in peripheral blood as small to medium lymphocytes with moderately abundant basophilic cytoplasm and characteristic short, unevenly distributed or polar villi (cytoplasmic projections)234. The presence of villous lymphocytes distinguishes SMZL from other small B-cell lymphomas and was historically used to describe this entity as "splenic lymphoma with circulating villous lymphocytes"4.
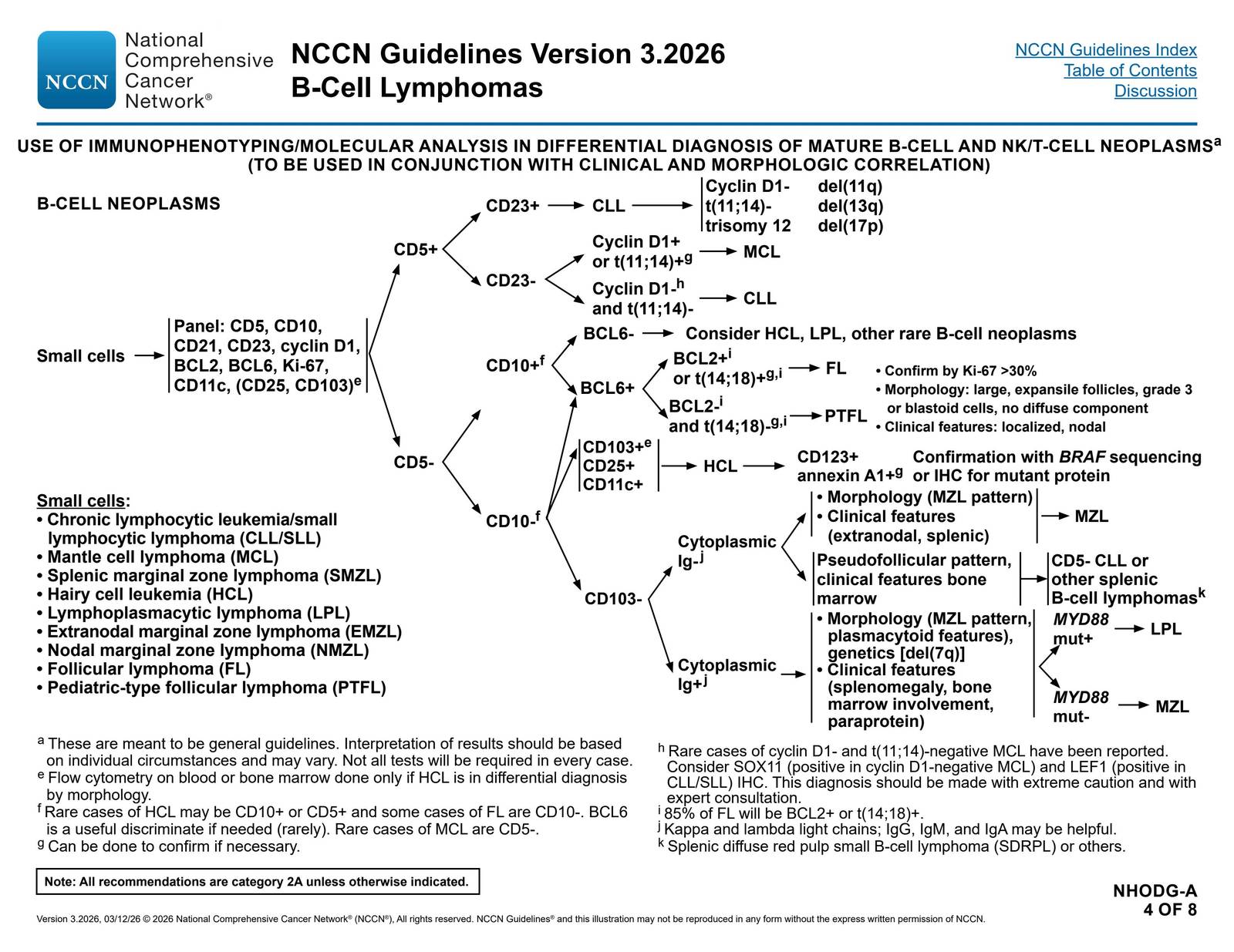
The immunophenotype is classic for SMZL. According to NCCN guidelines, the typical immunophenotype is CD10-, CD5-, CD20+, CD23-/+, CD43-/+, cyclin D1-, BCL2- follicles, annexin A1-, and CD103-1. This patient's profile (CD5-, CD20+, CD10-, CD43-, BCL2+) fits precisely. While a minority (≤5%) of SMZL cases may express CD5 or CD43, the typical case is negative for both markers24. The CD20+ expression confirms B-cell lineage, while the absence of CD5 and CD10 helps exclude CLL/SLL and follicular lymphoma, respectively1[^6].
The clinical presentation is pathognomonic: marked splenomegaly in the absence of peripheral lymphadenopathy is the defining clinical feature of SMZL12[^7]. Patients typically present in the 7th decade with findings of cytopenias, lymphocytosis, or splenomegaly (incidental or symptomatic)3. The bone marrow involvement >40% is consistent with SMZL, which characteristically shows nodular, interstitial, and/or intrasinusoidal infiltration patterns234.
2. Why the Other Options Are Less Likely¶
(A) Mantle cell lymphoma (MCL) is excluded by the CD5-negative immunophenotype. MCL is characteristically CD5+/CD23- with cyclin D1 overexpression or t(11;14) translocation[^6]. While rare CD5-negative MCL cases exist, they would require SOX11 positivity for diagnosis and should be made with extreme caution and expert consultation[^6]. The absence of CD5 makes MCL highly unlikely in this case.
(B) Hairy cell leukemia (HCL) is excluded by the negative CD103, CD25, CD123, and annexin A1 markers (implied by the CD5-/CD20+/CD10-/CD43-/BCL2+ profile without mention of HCL-specific markers). HCL characteristically expresses CD103+, CD25+, CD123+, and annexin A1+, with the genetic hallmark BRAF V600E mutation present in essentially all cases[7][9][^10]. HCL also typically presents with pancytopenia and marked monocytopenia, not the lymphocytosis described here[7][10]. The villous lymphocytes in SMZL have short polar villi, distinct from the thin circumferential projections ("hairy" appearance) of HCL[^10].
(D) Splenic follicular lymphoma is excluded by the CD10-negative immunophenotype. Follicular lymphoma is characteristically CD10+/BCL6+ with t(14;18) translocation in 85% of cases[^6]. While rare CD10-negative follicular lymphomas exist, BCL6 positivity would be expected[^6]. The CD10-negative status strongly argues against follicular lymphoma.
(E) Hepatosplenic lymphoma (hepatosplenic T-cell lymphoma) is excluded because this is a B-cell neoplasm (CD20+). Hepatosplenic T-cell lymphoma is a rare γδ T-cell lymphoma that presents with hepatosplenomegaly without lymphadenopathy, but would be CD3+/CD20-negative with a T-cell immunophenotype. The CD20+ expression definitively excludes this diagnosis.

詳解 · 中文翻譯¶
1. 為什麼 (C) 脾邊緣區淋巴瘤是正確的¶
脾邊緣區淋巴瘤 (SMZL) 是最可能的診斷,基於脾腫大無周邊淋巴結病變、周邊血中絨毛淋巴細胞和特徵性 CD5-/CD20+/CD10-/CD43-/BCL2+ 免疫表型的星座123。
絨毛淋巴細胞是 SMZL 的標誌性形態特徵。這些細胞在周邊血中出現為小至中等淋巴細胞,具有中等豐富的嗜鹼性細胞質和特徵性的短的、不均勻分佈或極性絨毛(細胞質突出)234。絨毛淋巴細胞的存在區分 SMZL 與其他小 B 細胞淋巴瘤,並且歷史上被用於描述此實體為「具有循環絨毛淋巴細胞的脾淋巴瘤」4。
免疫表型對 SMZL 是經典的。根據 NCCN 指南,典型免疫表型是 CD10-、CD5-、CD20+、CD23-/+、CD43-/+、cyclin D1-、BCL2- 濾泡、annexin A1- 和 CD103-1。此患者的檔案(CD5-、CD20+、CD10-、CD43-、BCL2+)精確符合。雖然少數(≤5%)SMZL 病例可表達 CD5 或 CD43,典型病例對兩個標誌都是陰性的24。CD20+ 表達確認 B 細胞世系,而 CD5 和 CD10 的缺失有助於分別排除 CLL/SLL 和濾泡淋巴瘤1[^6]。
臨床表現是病理症狀典型的:在無周邊淋巴結病變情況下明顯脾腫大是 SMZL 的定義臨床特徵12[^7]。患者通常在第 7 個十年中期出現,具有細胞減少症、淋巴細胞增多症或脾腫大(偶然或症狀性)的發現3。>40% 的骨髓受累與 SMZL 一致,其特徵性顯示結節性、間質性和/或血管竇內浸潤模式234。
2. 為什麼其他選項較不可能¶
(A) 套細胞淋巴瘤 (MCL) 被 CD5 陰性免疫表型排除。MCL 特徵性為 CD5+/CD23- 具有 cyclin D1 過度表達或 t(11;14) 易位[^6]。雖然罕見 CD5 陰性 MCL 病例存在,但它們需要 SOX11 陽性以進行診斷並應以極端謹慎和專家諮詢製作[^6]。CD5 的缺失使 MCL 在此病例中極不可能。
(B) 毛細胞白血病 (HCL) 被陰性 CD103、CD25、CD123 和 annexin A1 標誌排除(由 CD5-/CD20+/CD10-/CD43-/BCL2+ 檔案暗示,未提及 HCL 特異性標誌)。HCL 特徵性表達 CD103+、CD25+、CD123+ 和 annexin A1+,遺傳標誌BRAF V600E 突變存在於本質上所有病例中[7][9][^10]。HCL 也通常表現為全血細胞減少症和明顯單核細胞減少症,而不是此處描述的淋巴細胞增多症[7][10]。SMZL 中的絨毛淋巴細胞具有短極性絨毛,不同於 HCL 的薄周向投影(「毛髮樣」外觀)[^10]。
(D) 脾濾泡淋巴瘤被 CD10 陰性免疫表型排除。濾泡淋巴瘤特徵性為 CD10+/BCL6+ 具有 t(14;18) 易位於 85% 的病例中[^6]。雖然罕見 CD10 陰性濾泡淋巴瘤存在,BCL6 陽性性會被預期[^6]。CD10 陰性狀態強烈反對濾泡淋巴瘤。
(E) 肝脾淋巴瘤(肝脾 T 細胞淋巴瘤)被排除因為這是B 細胞腫瘤(CD20+)。肝脾 T 細胞淋巴瘤是罕見的 γδ T 細胞淋巴瘤,表現為肝脾腫大無淋巴結病變,但將是 CD3+/CD20- 陰性具有 T 細胞免疫表型。CD20+ 表達明確排除此診斷。
參考文獻 (AMA)¶
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=43. ↩↩↩↩↩↩↩↩
-
Blombery P, de Jong D, Ferry JA, et al. Closing the Gap Between Biology and Classification in Splenic B-Cell Lymphomas. Histopathology. 2025;86(1):69-78. doi:10.1111/his.15323. PMID:39403047. ↩↩↩↩↩↩↩↩↩↩
-
Porwit A, Fend F, Kremer M, et al. Issues in Diagnosis of Small B Cell Lymphoid Neoplasms Involving the Bone Marrow and Peripheral Blood. Report on the Bone Marrow Workshop of the XVIIth Meeting of the European Association for Haematopathology and the Society for Hematopathology. Histopathology. 2016;69(3):349-73. doi:10.1111/his.12999. PMID:27208429. ↩↩↩↩↩↩↩↩
-
Falini B, Tiacci E. Hairy-Cell Leukemia. The New England Journal of Medicine. 2024;391(14):1328-1341. doi:10.1056/NEJMra2406376. PMID:39383460. ↩↩↩↩↩↩↩↩
Figures¶