Q60. Which agent/regimen is not recommended as therapy for the patients with relapsed low grade follicular lymphomas?¶
- (A) Rituximab monotherapy
- (B) Rituximab plus lenalidomide
- (C) Rituximab plus bendamustine
- (D) Fludarabine-based therapy
- (E) EZH2 inhibitor (Tazemetostat)
點此顯示正解
(D) Fludarabine-based therapy
詳解¶
Analysis¶
1. Why (D) Fludarabine-based therapy is the INCORRECT (NOT recommended) statement:
Fludarabine-based therapy is NOT recommended for relapsed follicular lymphoma in the modern treatment era. While fludarabine showed activity in historical studies from the 1990s-2000s, it has been supplanted by safer, more effective, and less toxic regimens12. Current guidelines do not include fludarabine-based regimens as recommended options for relapsed follicular lymphoma2. The shift away from fludarabine reflects several concerns:
- Limited durability: Even in older studies, fludarabine monotherapy produced complete responses in only 20-40% of cases, with short progression-free survival (median 5.4 months in alkylator-resistant disease)89
- Significant toxicity: Fludarabine causes substantial myelosuppression, infectious complications, and neurologic toxicity (10% grade 3 neurologic events including visual and auditory changes)7[^10]
- Availability of superior alternatives: Modern chemotherapy-free regimens (lenalidomide-rituximab, bispecific antibodies, CAR T-cell therapy, EZH2 inhibitors) offer better efficacy with more favorable toxicity profiles12
The NCCN guidelines for relapsed follicular lymphoma do not list any fludarabine-containing regimens among preferred or other recommended options2.
2. Why the other options ARE recommended:
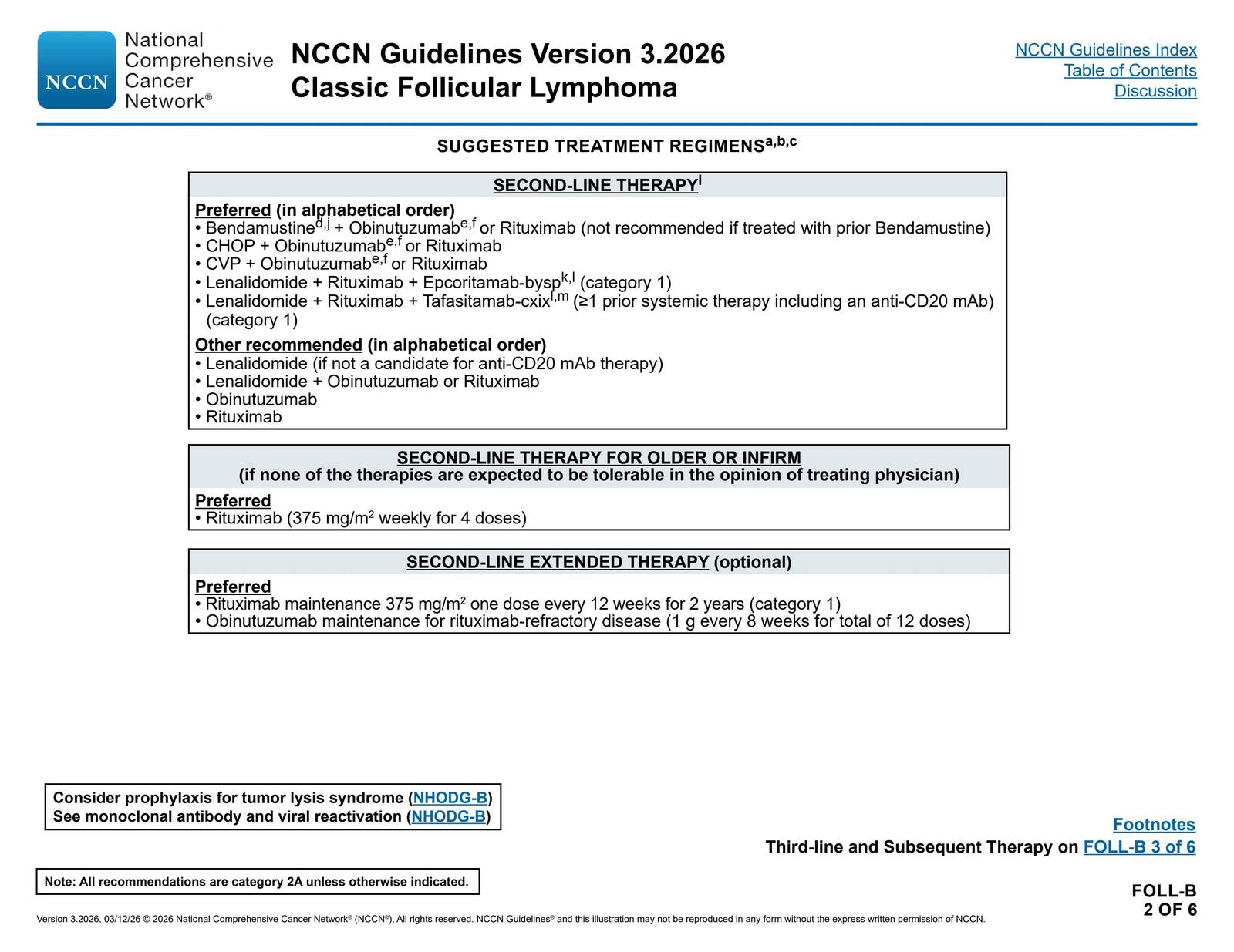
(A) Rituximab monotherapy is explicitly recommended by NCCN guidelines as "Other recommended" second-line therapy and as "Preferred" for older or infirm patients (375 mg/m² weekly for 4 doses)2. It provides a well-tolerated option with established efficacy2.
(B) Rituximab plus lenalidomide (R²) is a cornerstone of relapsed follicular lymphoma treatment, listed as "Other recommended" by NCCN2. This chemotherapy-free combination is "an internationally accepted standard" for relapsed/refractory disease after at least one prior line5. Recent phase 3 trials (AUGMENT, inMIND, EPCORE FL-1) have validated its efficacy, with enhanced outcomes when combined with tafasitamab or epcoritamab45.
(C) Rituximab plus bendamustine is a "Preferred" regimen in NCCN guidelines for second-line therapy (bendamustine + obinutuzumab or rituximab), though not recommended if previously treated with bendamustine2. This combination represents one of the most widely used chemoimmunotherapy approaches for relapsed disease3.
(E) EZH2 inhibitor (Tazemetostat) is FDA-approved and recommended for relapsed follicular lymphoma. It is "the first approved epigenetic-directed therapy" with overall response rates of 69% in EZH2-mutated patients and 35% in wild-type EZH21. Tazemetostat is offered to patients with ≥2 prior treatments who carry EZH2 mutations or have no other therapeutic options1.
詳解 · 中文翻譯¶
1. 為什麼 (D) Fludarabine 為主的治療是錯誤的(不推薦的)敘述:
Fludarabine 為主的治療不推薦用於現代治療時代中復發的濾泡性淋巴瘤。儘管 fludarabine 在 1990 年代至 2000 年代的歷史研究中顯示活性,它已被更安全、更有效且毒性更低的治療方案取代12。當前指南不將 fludarabine 為主的方案列為復發性濾泡性淋巴瘤的推薦選項2。遠離 fludarabine 的轉變反映了多個考慮:
- 耐久性有限:即使在較舊的研究中,fludarabine 單藥治療也僅在 20-40% 的病例中產生完全緩解,無進展生存期短(在鹼化劑耐受疾病中中位 5.4 個月)89
- 顯著毒性:Fludarabine 導致重度骨髓抑制、感染並發症及神經毒性(10% 三級神經事件,包括視覺和聽覺改變)7[^10]
- 優越替代方案的可用性:現代無化療方案(lenalidomide-rituximab、雙特異性抗體、CAR T 細胞治療、EZH2 抑制劑)提供更好的療效和更有利的毒性特徵12
復發性濾泡性淋巴瘤的 NCCN 指南未在首選或其他推薦選項中列出任何含 fludarabine 的方案2。
2. 為什麼其他選項都推薦:
(A) Rituximab 單藥治療被 NCCN 指南明確推薦為「其他推薦的」二線治療,對於年長或體弱患者為「首選」(375 mg/m² 每週一次,共 4 次)2。它提供良好耐受性和既定療效的選項2。
(B) Rituximab 加 lenalidomide (R²)是復發性濾泡性淋巴瘤治療的基石,被 NCCN 列為「其他推薦的」2。此無化療聯合是在至少一個先前治療後用於復發/難治疾病的「國際接受的標準」5。最近的三期試驗(AUGMENT、inMIND、EPCORE FL-1)驗證了其療效,與 tafasitamab 或 epcoritamab 聯合時有增強的療效45。
(C) Rituximab 加 bendamustine 是 NCCN 指南中二線治療的「首選」方案(bendamustine + obinutuzumab 或 rituximab),但如果之前已用 bendamustine 治療則不推薦2。此聯合代表復發疾病中最廣泛使用的化免聯合方法之一3。
(E) EZH2 抑制劑(Tazemetostat)已 FDA 批准並推薦用於復發性濾泡性淋巴瘤。它是「首個批准的表觀遺傳學導向治療」,在 EZH2 突變患者中總緩解率為 69%,在野生型 EZH2 中為 35%1。Tazemetostat 提供給至少接受過 2 次先前治療且携帶 EZH2 突變或無其他治療選項的患者1。
參考文獻 (AMA)¶
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩↩↩↩↩↩↩
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=23. ↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩↩
-
Lenz G, Hiddemann W, Dreyling M. The Role of Fludarabine in the Treatment of Follicular and Mantle Cell Lymphoma. Cancer. 2004;101(5):883-93. doi:10.1002/cncr.20483. PMID:15329894. ↩↩
-
Tinmouth A, Zanke B, Imrie KR. Fludarabine in Alkylator-Resistant Follicular Non-Hodgkin's Lymphoma. Leukemia & Lymphoma. 2001;41(1-2):137-45. doi:10.3109/10428190109057962. PMID:11342365. ↩↩
-
Anderson VR, Perry CM. Fludarabine: A Review of Its Use in Non-Hodgkin's Lymphoma. Drugs. 2007;67(11):1633-55. doi:10.2165/00003495-200767110-00008. PMID:17661532. ↩↩↩↩
-
Hochster HS, Kim KM, Green MD, et al. Activity of Fludarabine in Previously Treated Non-Hodgkin's Low-Grade Lymphoma: Results of an Eastern Cooperative Oncology Group Study. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 1992;10(1):28-32. doi:10.1200/JCO.1992.10.1.28. PMID:1727921. ↩
-
Falchi L, Nijland M, Huang H, et al. Epcoritamab, Lenalidomide, and Rituximab Versus Lenalidomide and Rituximab for Relapsed or Refractory Follicular Lymphoma (EPCORE FL-1): A Global, Open-Label, Randomised, Phase 3 Trial. Lancet (London, England). 2026;407(10524):161-173. doi:10.1016/S0140-6736(25)02360-8. PMID:41371238. ↩↩
-
Sehn LH, Hübel K, Luminari S, et al. Tafasitamab, Lenalidomide, and Rituximab in Relapsed or Refractory Follicular Lymphoma (inMIND): A Global, Phase 3, Randomised Controlled Trial. Lancet (London, England). 2026;407(10524):133-146. doi:10.1016/S0140-6736(25)01778-7. PMID:41360064. ↩↩
-
Armitage JO, Gascoyne RD, Lunning MA, Cavalli F. Non-Hodgkin Lymphoma. Lancet (London, England). 2017;390(10091):298-310. doi:10.1016/S0140-6736(16)32407-2. PMID:28153383. ↩↩
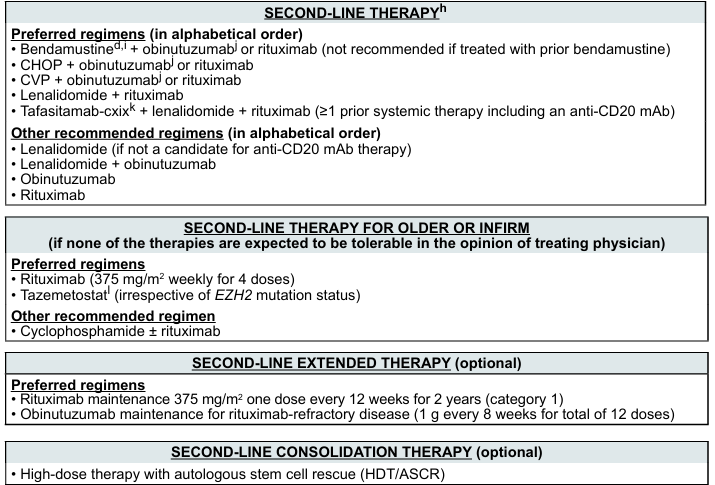
Slide annotations
The slide contains a table listing preferred and other recommended regimens for second-line therapy, second-line therapy for older or infirm patients, extended therapy, and consolidation therapy for relapsed low-grade follicular lymphomas.
Figures¶