Q1. Which one of the followings is WRONG regarding Follicular Lymphoma (FL)?¶
- (A) Express CD10, CD19, CD20, CD22, CD79a, and surface Ig.
- (B) FL cells typically express BCL-2, and BCL-6.
- (C) FL is graded based on the number of centrocytes / HPF.
- (D) FL grades 3a is an aggressive disease.
- (E) Cytogenetic changes t(14;18) causes overexpression of the anti-apoptotic BCL-2 protein.
點此顯示正解
(C) FL is graded based on the number of centrocytes / HPF.
詳解¶
Analysis¶
1) Why (C) is the WRONG statement:
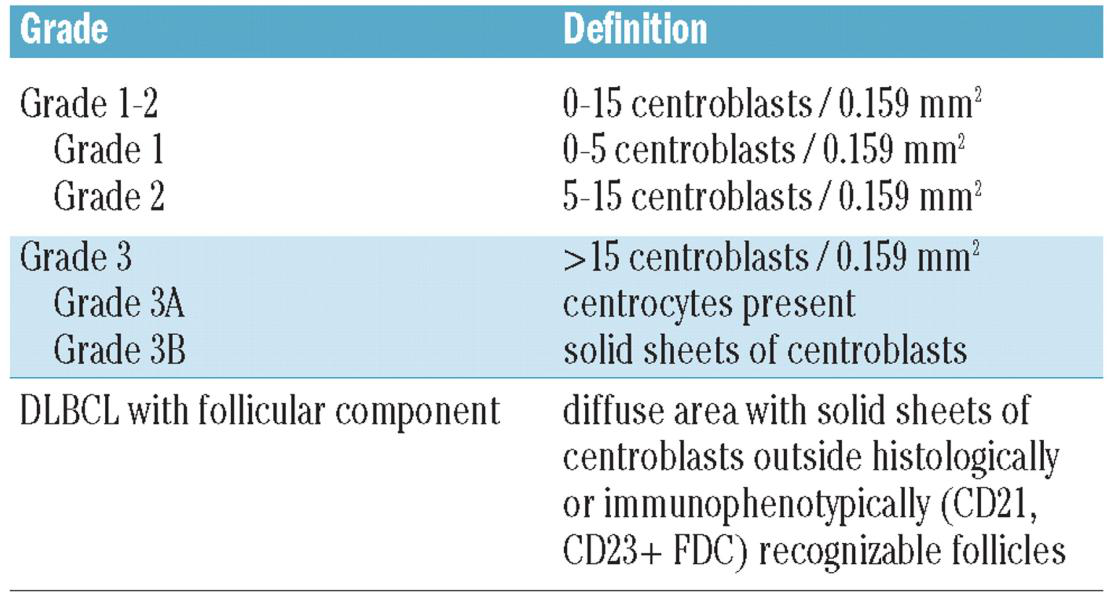
Option (C) states that "FL is graded based on the number of centrocytes / HPF" — this is incorrect. Follicular lymphoma is graded based on the number of centroblasts (large transformed cells), not centrocytes (small cleaved cells), per high-power field136. The grading system (grades 1, 2, 3A, and 3B) depends on counting centroblasts to distinguish indolent from more aggressive disease. Centrocytes are the small cleaved follicle center cells that, along with centroblasts, comprise the neoplastic follicles, but they are not the basis for grading16.
2) Why the other options are TRUE:
(A) Express CD10, CD19, CD20, CD22, CD79a, and surface Ig — TRUE. FL cells are positive for these B-cell markers in virtually all cases. The typical immunophenotype includes CD19, CD20, CD22, CD79a, CD10 (in most cases), and monoclonal surface immunoglobulin58[9][10]. The NCCN guidelines confirm this typical immunophenotype: CD10+, CD20+, BCL2+, BCL6+5.
(B) FL cells typically express BCL-2 and BCL-6 — TRUE. BCL-2 protein is strongly positive in almost all patients with grades 1-2 FL, and BCL-6 is expressed by at least some neoplastic cells in all FL tumors78[^9]. This dual expression (BCL-2 and BCL-6) is characteristic of the germinal center origin of FL cells57.
(D) FL grades 3A is an aggressive disease — TRUE (though this is somewhat controversial). While the management of FL3A is described as "controversial" and should be "individualized"5, recent evidence demonstrates that FL3A behaves more aggressively than FL grades 1-2. A 2025 study showed FL3A shares clinical characteristics with the aggressive group (FL3B and FL/DLBCL) rather than the indolent FL1-2 group4. The WHO classification groups FL3A with classic FL, but clinically it demonstrates more aggressive behavior than lower grades134.
(E) Cytogenetic changes t(14;18) causes overexpression of the anti-apoptotic BCL-2 protein — TRUE. The t(14;18)(q32;q21) translocation is the characteristic molecular hallmark of FL, occurring in approximately 60-90% of cases678[9][10]. This translocation juxtaposes the BCL2 gene with the immunoglobulin heavy chain (IgH) locus, resulting in constitutive overexpression of the anti-apoptotic BCL-2 protein167.
詳解 · 中文翻譯¶
分析¶
1) 為何 (C) 是錯誤陳述:
選項 (C) 指出「濾泡淋巴瘤根據中等淋巴球 / HPF 的數量分級」——這是不正確的。濾泡淋巴瘤根據大淋巴母細胞(大轉化細胞)的數量分級,而非中等淋巴球(小裂隙細胞),每高倍視野136。分級系統(第 1、2、3A 和 3B 級)取決於計算大淋巴母細胞以區分惰性與更具侵襲性疾病。中等淋巴球是與大淋巴母細胞一起組成腫瘤性濾泡的小裂隙濾泡中心細胞,但它們不是分級的基礎16。
2) 其他選項為何真實:
(A) 表達 CD10、CD19、CD20、CD22、CD79a 和表面 Ig — 真實。FL 細胞在幾乎所有情況下都對這些 B 細胞標誌物陽性。典型的免疫表型包括 CD19、CD20、CD22、CD79a、CD10(在大多數情況下)和單克隆表面免疫球蛋白58[9][10]。NCCN 指南確認此典型免疫表型:CD10+、CD20+、BCL2+、BCL6+5。
(B) FL 細胞通常表達 BCL-2 和 BCL-6 — 真實。BCL-2 蛋白在幾乎所有 1-2 級 FL 患者中強陽性,BCL-6 在所有 FL 腫瘤中至少由某些腫瘤細胞表達78[^9]。這種雙重表達(BCL-2 和 BCL-6)是 FL 細胞生髮中心來源的特徵57。
(D) FL 第 3A 級是侵襲性疾病 — 真實(雖然這在某種程度上有爭議)。雖然 FL3A 的管理被描述為「有爭議」且應「個體化」5,但最近的證據顯示 FL3A 的行為比 FL 1-2 級更具侵襲性。一項 2025 年的研究顯示 FL3A 與侵襲性組(FL3B 和 FL/DLBCL)共享臨床特徵,而非惰性 FL1-2 組4。WHO 分類將 FL3A 與經典 FL 分組,但臨床上它表現出比較低等級更具侵襲性的行為134。
(E) 細胞遺傳學變化 t(14;18) 導致抗凋亡 BCL-2 蛋白的過度表達 — 真實。t(14;18)(q32;q21) 易位是 FL 的特徵性分子標記,發生在約 60-90% 的病例中678[9][10]。此易位將 BCL2 基因與免疫球蛋白重鏈(IgH)位點並置,導致抗凋亡 BCL-2 蛋白的組成型過度表達167。
參考文獻 (AMA)¶
-
Silkenstedt E, Salles G, Campo E, Dreyling M. B-Cell Non-Hodgkin Lymphomas. Lancet (London, England). 2024;403(10438):1791-1807. doi:10.1016/S0140-6736(23)02705-8. PMID:38614113. ↩↩↩↩↩↩↩↩
-
Armitage JO, Gascoyne RD, Lunning MA, Cavalli F. Non-Hodgkin Lymphoma. Lancet (London, England). 2017;390(10091):298-310. doi:10.1016/S0140-6736(16)32407-2. PMID:28153383. ↩
-
National Comprehensive Cancer Network. B-Cell Lymphomas. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf#page=15. ↩↩↩↩
-
Dada R. Diagnosis and Management of Follicular Lymphoma: A Comprehensive Review. European Journal of Haematology. 2019;103(3):152-163. doi:10.1111/ejh.13271. PMID:31270855. ↩↩↩↩
-
Freedman A, Jacobsen E. Follicular Lymphoma: 2020 Update on Diagnosis and Management. American Journal of Hematology. 2020;95(3):316-327. doi:10.1002/ajh.25696. PMID:31814159. ↩↩↩↩↩↩↩↩
-
Freedman A. Follicular Lymphoma: 2018 Update on Diagnosis and Management. American Journal of Hematology. 2018;93(2):296-305. doi:10.1002/ajh.24937. PMID:29314206. ↩↩↩↩↩↩↩↩
-
Marafioti T, Copie-Bergman C, Calaminici M, et al. Another Look at Follicular Lymphoma: Immunophenotypic and Molecular Analyses Identify Distinct Follicular Lymphoma Subgroups. Histopathology. 2013;62(6):860-75. doi:10.1111/his.12076. PMID:23509938. ↩↩↩↩↩↩↩↩
-
Sun C, Li W, Yu J, et al. Molecular Landscape of Distinct Follicular Lymphoma Histologic Grades: Insights From Genomic and Transcriptome Analyses. Leukemia. 2025;39(6):1425-1434. doi:10.1038/s41375-025-02603-9. PMID:40234612. ↩↩↩↩↩↩
Slide annotations
Centroblast
Figures¶