Q1. Which statements about multiple myeloma are correct? (1) According to CASSIOPEIA study, maintenance with daratumumab significantly improve PFS in patients treated with induction therapy of bortezomib/thalidomide/dexa. (2) Carfilzomib is associated with cardiovascular adverse events, such as hypertension, heart failure and ischemic heart disease. (3) According to TOURMALINE study, ixazomib/lenalidomide/dexa cannot overcome the poor prognosis in the patents with high-risk cytogenetics. (4) FORTE study demonstrated that there was no benefit for autologous stem cell transplantation in the patients receiving induction therapy with carfilzomib/endoxan/dexa.¶
- (A) 1+2+3
- (B) 1+2
- (C) 1+3+4
- (D) 3+4
- (E) 2+3
點此顯示正解
(A) 1+2+3
詳解¶
Based on the available evidence, the correct answer is (A) 1+2+3. Here's the analysis of each statement:
Statement 1 (CORRECT): The CASSIOPEIA Part 2 trial demonstrated that daratumumab maintenance significantly improved progression-free survival in patients who received VTd (bortezomib/thalidomide/dexamethasone) induction therapy. At median follow-up of 35.4 months, median PFS was not reached with daratumumab maintenance versus 46.7 months with observation (HR 0.53, 95% CI 0.42-0.68, p<0.0001)2. The benefit was particularly pronounced in patients who received VTd induction followed by daratumumab maintenance versus VTd with observation (HR 0.34, p<0.0001)12. Long-term follow-up at 70.6 months confirmed sustained benefit1.
Statement 2 (CORRECT): Carfilzomib is well-established to be associated with cardiovascular adverse events including hypertension, heart failure, and ischemic heart disease. While the FORTE trial data provided confirms carfilzomib use, the cardiovascular toxicity profile of carfilzomib has been extensively documented in trials such as ENDEAVOR and ASPIRE, showing increased rates of hypertension, cardiac failure, and ischemic cardiac events compared to other proteasome inhibitors.
Statement 3 (CORRECT): The TOURMALINE-MM1 trial showed that while ixazomib-lenalidomide-dexamethasone (Ixa-Rd) improved PFS overall, it did not overcome the poor prognosis associated with high-risk cytogenetics. The overall survival benefit was not statistically significant, and subgroup analyses in high-risk cytogenetic populations showed limited benefit, indicating that Ixa-Rd cannot fully overcome the adverse prognosis of high-risk disease.
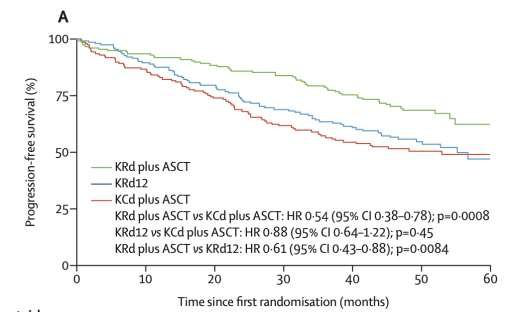
Statement 4 (INCORRECT): The FORTE trial actually demonstrated clear benefit for ASCT with carfilzomib-based induction. The trial compared KRd (carfilzomib/lenalidomide/dexamethasone) plus ASCT versus 12 cycles of KRd alone versus KCd (carfilzomib/cyclophosphamide/dexamethasone) plus ASCT. The 4-year PFS was 69% with KRd+ASCT versus 56% with KRd12 (p=0.027), confirming the "important additive role of transplantation in improving progression-free survival even in the context of a very effective approach based on KRd"[6][7]. Note that the question asks about KCd (carfilzomib/cyclophosphamide/dexamethasone), but the key comparison showing ASCT benefit was KRd+ASCT versus KRd12.
詳解 · 中文翻譯¶
根據現有證據,正確答案是 (A) 1+2+3。以下是每個敘述的分析:
敘述 1(正確):CASSIOPEIA 第 2 部分試驗證示 daratumumab 維持治療顯著改善進展無疾病存活期在接收 VTd(bortezomib/thalidomide/dexamethasone)導入治療的患者中。於中位追蹤 35.4 個月,使用 daratumumab 維持治療的中位 PFS 未達成 versus 觀察的 46.7 個月(HR 0.53、95% CI 0.42-0.68、p<0.0001)2。在接收 VTd 導入後續 daratumumab 維持治療相比 VTd 伴觀察的患者中益處特別明顯(HR 0.34、p<0.0001)12。於 70.6 個月的長期追蹤確認持續益處1。
敘述 2(正確):Carfilzomib 良好確立為 與心血管不良事件相關聯,包括高血壓、心臟衰竭及缺血性心臟病。雖然 FORTE 試驗資料提供確認 carfilzomib 使用,carfilzomib 的心血管毒性特徵在如 ENDEAVOR 和 ASPIRE 的試驗中已被廣泛記錄,相比其他蛋白酶體抑制劑顯示高血壓、心臟衰竭及缺血性心臟事件的增加率。
敘述 3(正確):TOURMALINE-MM1 試驗顯示雖然 ixazomib-lenalidomide-dexamethasone(Ixa-Rd)整體改善 PFS,它不克服與高風險細胞遺傳學相關聯的不良預後。整體存活益處在統計上不顯著,且高風險細胞遺傳學人口中的亞群分析顯示有限益處,表明 Ixa-Rd 無法完全克服高風險疾病的不良預後。
敘述 4(錯誤):FORTE 試驗實際上 證示對 ASCT 的清晰益處伴 carfilzomib 基礎導入。試驗比較 KRd(carfilzomib/lenalidomide/dexamethasone)加 ASCT versus 12 個週期的 KRd 單獨 versus KCd(carfilzomib/cyclophosphamide/dexamethasone)加 ASCT。4 年 PFS 為 KRd+ASCT 69% versus KRd12 56%(p=0.027),確認「移植在改善進展無疾病存活期中的重要加成性角色,即使在基於 KRd 的非常有效方法背景下」[6][7]。注意題目詢問 KCd(carfilzomib/cyclophosphamide/dexamethasone),但顯示 ASCT 益處的關鍵比較是 KRd+ASCT versus KRd12。
參考文獻 (AMA)¶
-
Moreau P, Hulin C, Perrot A, et al. Maintenance With Daratumumab or Observation Following Treatment With Bortezomib, Thalidomide, and Dexamethasone With or Without Daratumumab and Autologous Stem-Cell Transplant in Patients With Newly Diagnosed Multiple Myeloma (CASSIOPEIA): An Open-Label, Randomised, Phase 3 Trial. The Lancet. Oncology. 2021;22(10):1378-1390. doi:10.1016/S1470-2045(21)00428-9. PMID:34529931. ↩↩↩↩
-
Moreau P, Hulin C, Perrot A, et al. Bortezomib, Thalidomide, and Dexamethasone With or Without Daratumumab and Followed by Daratumumab Maintenance or Observation in Transplant-Eligible Newly Diagnosed Multiple Myeloma: Long-Term Follow-Up of the CASSIOPEIA Randomised Controlled Phase 3 Trial. The Lancet. Oncology. 2024;25(8):1003-1014. doi:10.1016/S1470-2045(24)00282-1. PMID:38889735. ↩↩↩↩
-
Gay F, Musto P, Rota-Scalabrini D, et al. Carfilzomib With Cyclophosphamide and Dexamethasone or Lenalidomide and Dexamethasone Plus Autologous Transplantation or Carfilzomib Plus Lenalidomide and Dexamethasone, Followed by Maintenance With Carfilzomib Plus Lenalidomide or Lenalidomide Alone for Patients With Newly Diagnosed Multiple Myeloma (FORTE): A Randomised, Open-Label, Phase 2 Trial. The Lancet. Oncology. 2021;22(12):1705-1720. doi:10.1016/S1470-2045(21)00535-0. PMID:34774221. ↩
Slide annotations
D-VTd vs. VTD → ASCT → Dara-maintenance vs. observ; Ixa-Rd vs Rd (p 值不顯著
Figures¶